The EMS provider with the highest level of certification is ultimately responsible for the initial assessment of all patients unless
the number of patients and/or severity of injuries makes this impossible.
In the event of a non-transport (refusal or non-viability), the EMS provider with the highest level of certification is responsible
for the assessment and documentation unless the number of patients and/or severity of injuries makes it impossible.
In a situation where a BLS crew has requested a paramedic (ALS) for assistance and the paramedic feels BLS transport is indicated,
the paramedic will continue to assist the BLS crew throughout the transport.
ALS assessment, treatment, and transport is indicated if the patient has one or more of the following conditions:
Shortness of breath
Chest pain or angina equivalent or chest pain that could be cardiac in nature
New onset altered level of consciousness
Uncontrollable bleeding (this includes initially uncontrolled bleeding, that is now controlled)
Acute onset of fatigue and/or diaphoresis in patients with past cardiac history
Unconsciousness
Seizures
Patients who meet Trauma Alert/Stabilization Room criteria
Patients who meet Medical Alert/Stabilization Room criteria
Shock signs and/or symptoms (unstable patient)
Syncope or near-syncope
Any uncertainty about the patient’s status
Any transport with physician, PA, NP or NNP attending or accompanying.
Anytime the EMS provider(s) believe the patient’s condition warrants ALS assessment, treatment, and transport
Patient care may be delegated from the paramedic to the EMT under the following conditions:
The patient is stable and does not meet any of the criteria for ALS transport listed above.
The paramedic fully informs the EMT of assessment findings and anticipated patient needs.
The EMT is comfortable and accepting responsibility for treatment and transport.
The patient has not received any ALS treatment (i.e.-IV therapy, intubation, RX, etc.).
The paramedic fully documents assessment findings and treatment up to the point of delegation of patient care to the EMT.
If a BLS crew is able to deliver the patient to an emergency department in less time than it would take for an ALS crew to make
contact, the BLS crew should complete the transport. Waiting for ALS to arrive should not cause delays in transporting the
patient.
Approved: 14 May 2021
Approved: 14 May 2021
Ridgeview Ambulance Protocols
Operations
0200
Radio Report Format
0200 - Radio Report Format
The following formats for presentation of patient reports were developed to provide order and consistency for
system ambulance personnel when presenting reports to receiving facilities. The order of information has been developed to attempt to meet
the most common communication practices among crews and the needs of medical control physicians and other hospital staff members.
When relaying patient information via radio for a patient report or medical control, ambulance crews will provide the following information
in the order given immediately upon departure from the scene:
Radio Report Format
When relaying patient information via face-to-face hand-off of a patient, ambulance crews will provide the following information in the
order given:
Verbal Hand-off Report Format
Updated: 9 April 2025
Updated: 9 April 2025
Ridgeview Ambulance Protocols
Operations
0300
Service Animals
0300 - Service Animals
PURPOSE:
It is the policy of Ridgeview Medical Center (RMC) to comply with the requirements of the American with Disabilities Act,
as amended, and the Department of Justice’s implementing regulation Section 504 of the Rehabilitation Act 1073, as amended,
that broadest access be provided to service animals and that persons using service animals be afforded independent access
to the Hospital. Except as specified below, it is anticipated that a person using a service animal shall generally be afforded
the same access to the Hospital as that afforded the public in general.
DEFINITIONS:
Disability: An “individual with a disability” means a person who has a physical or mental impairment that
substantially impairs one or major life activities including, but not limited to:
walking
talking
seeing
breathing
hearing
Service Animal: Under the ADA, a service animal is defined as a dog that has been individually trained to do work
or perform tasks for an individual with a disability. The task(s) performed by the dog must be directly related to the
person's disability.
Specific Action for Disability: The dog must be trained to take a specific action when needed to assist
the person with a disability. For example, a person with diabetes may have a dog that is trained to alert him when
his blood sugar reaches high or low levels. A person with depression may have a dog that is trained to remind her to
take her medication. Or, a person who has epilepsy may have a dog that is trained to detect the onset of a seizure
and then help the person remain safe during the seizure.
Dog Breed: The ADA does not restrict the type of dog breeds that can be service animals.
Physical Identifiers: The ADA does not require service animals to wear a vest, ID tag, or specific
harness.
Therapy Animals: Are not service animals and are not entitled to the same access that must be given
by law to service animals, as they have not been individually trained to perform disability mitigating tasks.
Safety/Health: A service animal may not be excluded based on assumptions or stereotypes about the animal's breed or
how the animal might behave. However, if a particular service animal behaves in a way that poses a direct threat to the
health or safety of others, has a history of such behavior, or is not under the control of the handler, that animal may
be excluded. If an animal is excluded for such reasons, staff must still offer their goods or services to the person
without the animal present.
Direct Threat: A significant risk to the health or safety of others that cannot be eliminated or
mitigated by a modification of policies, practices, or procedures, or by the provision of auxiliary aids or
services. In determining whether a service animal poses a direct threat to the health or safety of others, RMC shall
make an individualized assessment, based on reasonable judgment that relies on current medical knowledge or on the
best available objective evidence, to ascertain:
the nature, duration, and severity of the risk;
the probability that a potential injury will actually occur;
whether reasonable modifications of policies, practices, or procedures will mitigate risk.
Aggression/Threat: Aggression in dogs commonly includes body language or threat displays such as a hard
stare, growling, barking, snarling, lunging, snapping, and/or biting.
Out of Control Animal: The ADA requires that service animals be under the control of the handler at all times. The
ADA does not require covered entities to modify policies, practices, or procedures if it would “fundamentally alter” the
nature of the goods, services, programs, or activities provided to the public. Nor does it overrule legitimate safety
requirements. If admitting service animals would fundamentally alter the nature of a service or program, service animals
may be prohibited. In addition, if a particular service animal is out of control and the handler does not take effective
action to control it, or if it is not housebroken, that animal may be excluded.
PROCEDURE:
In situations where it is not obvious that the dog is a service animal, staff may ask only two specific questions:
Is the dog a service animal required because of a disability?
What work or task has the dog been trained to perform?
Staff are not allowed to:
request any documentation for the dog
require that the dog demonstrate its task
inquire about the nature of the person's disability
Crews must also determine if there is a Direct Threat - significant risk to the health or safety of others?
Documentation: Use of a service animal shall be documented in the patient’s medical record including information regarding
areas in which the animal has been restricted.
References: ADA Service Animal Q&A; VCA - Aggression in Dogs;
United States Code. Title 42,Code 12101 – American with Disabilities act (ADA) 29 D.F.R. Part 36;
Sehulster, L. “Guideline for Environmental Infection Control in Healthcare Faculties, 2003.”
Zone 4 : Broadway St E and Adams Ave - Broadway St E & Adams Ave, New Germany, MN 55367 Satelite Image
Zone 5 : Hamburg Bicentennial Park - 614 Park Ave, Hamburg, MN 55339 Satelite Image
Zone 6 : Ridgeview Arlington Campus - 601 W Chandler St, Arlington, MN 55307 Satelite Image
Zone 7 : Ridgeview Le Sueur Campus - 621 S Fourth St, Le Sueur, MN 56058 Satelite Image
Zone 8 : Belle Plaine Athletic Complex (Parking Lot) - 1101 Commerce Dr W, Belle Plaine, MN 56011Satelite Image
Zone 9 : Scott County Fair Grounds - 7151 - 190th St W, Jordan, MN 55352Satelite Image
Zone 10 : Delano Emagine Movie Theater (Parking Lot) - 4423 US Highway 12, Delano, MN 55328Satelite Image
Zone 11 : Watertown Fire Department (Parking Lot) - 401 Carter St NE, Watertown, MN 55388Satelite Image
Zone 12 : Mayer Fire Department (Parking Lot) - 409 Shimmcor St, Mayer, MN 55360Satelite Image
Zone 13 : NYA Friendship Park - 316 - 4th Ave, Norwood Young America, MN 55397Satelite Image
Zone 14 : Cologne Security Bank & Trust (Parking Lot) - 1110 Village PKWY, Cologne, MN 55322Satelite Image
Revision Date: 15 February 2026
Revision Date: 15 February 2026
Ridgeview Ambulance Protocols
Operations
0600
Hospital Entry Codes
0600 - Hospital Entry Codes
Hospital
Door Code
Revision Date: 21 July 2024
Revision Date: 21 July 2024
Ridgeview Ambulance Protocols
Operations
0700
Clinical Timeout Policy
0700 - Clinical Timeout Policy
Policy Purpose: If providers cannot come to an agreement on a clinical intervention and one of the providers believe that
the proposed intervention is not appropriate and/or could negatively impact the health or wellbeing of the patient, a "clinical timeout"
should be called, immediately ceasing that intervention until medical control is contacted to determine the most appropriate course of
care.
Proceedure:
If a provider believes that a proposed intervention is not appropriate and could negatively impact the health or wellbeing of a patient
a "clinical timeout" will be called.
After a "clinical timeout" is called, the intervention in question will immediately cease while the crew continues to provide all other
appropriate cares.
The attending paramedic will contact medical control to discuss the case, the proposed intervention, and will allow medical control to
determine the best course of action.
The crew will follow the recommendation of medical control and will continue care as ordered.
The clinical timeout policy should only be used in cases where it is believed that a given intervention will have a significant negative
impact on the patient's health or wellbeing and the difference can't be reconciled by the providers. At no time should the clinical timeout
negate or delay any lifesaving intervention i.e. chest compressions, defibrillation, ventillation, etc. Medical control has the final
authority to determine the most appropriate course of care which must be followed by the crew. No provider (i.e. paramedic, supervisor,
manager, etc.) has the authority to override a clinical timeout, and once requested, must adhear to the outline procedure above.
The goal of prehospital emergency medical services is to deliver a viable patient to appropriate definitive care as soon as
possible. Optimal prehospital care results from a combination of careful patient assessment, essential prehospital emergency medical
services and appropriate medical consultation.
These BLS Patient Care Guidelines were developed to standardize the emergency patient care that EMS providers, through medical
consultation, deliver at the scene of illness or injury and while transporting the patient to the closest appropriate hospital. These
guidelines will help EMS providers anticipate and be better prepared to give the emergency patient care ordered during the medical
consultation.
As Medical Director for Ridgeview Medical Center Ambulance Service, I approve and adopt these guidelines for use in all patient care
encounters.
Signatures of Directors
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1050
ROLES and RESPONSIBILITIES of the MEDICAL DIRECTOR
1050 - ROLES and RESPONSIBILITIES of the MEDICAL DIRECTOR
Definition:
The Medical Director is a physician who accepts responsibility for the quality of care provided by drivers and attendants of a
Basic Life Support transportation service that has been granted a variance to perform a restricted treatment of procedure.
Requirements:
Pursuant to Minnesota Statute 144E.265 Subd. 1. The Medical Director must meet the following requirements:
be currently licensed as a physician in this state;
have experience in, and knowledge of, emergency care of acutely ill or traumatized patients; and
be familiar with the design and operation of local, regional, and state emergency medical service systems.
Roles and Responsibilities:
Pursuant to Minnesota Statute 144E.265 Subd. 2. The Medical Director responsibilities include but are not limited to:
Approving standards for training and orientation of personnel that impact patient care.
Approving standards for purchasing equipment and supplies that impact patient care.
Establishing standing orders for prehospital care.
Approving written triage, treatment, and transportation guidelines for adult and pediatric patients.
Participating in the development and operation of continuous quality improvement programs including, but not limited to,
case review and resolution of patient complaints.
Establishing procedures for the administration of drugs.
Maintaining the quality of care according to the standards and procedures established under clauses A through F.
Annual Assessment of EMTs:
Pursuant to Minnesota Statute144E.265 Subd. 3. Annually, the medical director or the medical director's designee
shall assess the practical skills of each person on the ambulance service roster and sign a statement verifying the proficiency
of each person.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1075
SERVICE RESPONSIBILITIES
1075 - SERVICE RESPONSIBILITIES
INSERT Service Specific Guideline
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1100
SCOPE
1100 - SCOPE
These Patient Care Guidelines apply to BLS ambulance services.
The following guidelines are to be used as consultative information to strive for the optimal care of patients. The statements
contained herein are intended to be informative and represent what is believed to be the current standard of care for any
particular circumstance. It is recognized that any specific procedure or recommendation is subject to modification depending
on circumstances of a particular case.
Age limits for pediatric and adult medical protocols must be flexible. For ages less than 13 years, pediatric orders should always
apply. Between the ages of 13 and 18, judgment should be used, although the pediatric orders will usually apply. Adult guidelines
apply to patient’s ages 18 and over. It is recognized that the exact age of a patient is not always known.
Courtesy to the patient, the patient's family, and other emergency care personnel is of utmost importance. Providing quality
patient care includes bringing any of the patient’s medication vials along with them when they are transported to a hospital or
other facility.
Minnesota Statutes, Chapter 144E.123 PREHOSPITAL CARE DATA. Requires the following: Subdivision 1. Collection and
maintenance. A licensee shall collect and provide prehospital care data to the board in a manner prescribed by the board. At a
minimum, the data must include items identified by the board that are part of the National Uniform Emergency Medical Services Data
Set. A licensee shall maintain prehospital care data for every response. Subdivision 2. Copy to receiving hospital. If a
patient is transported to a hospital, a copy of the ambulance report delineating prehospital medical care given shall be provided
to the receiving hospital.
The specific conditions listed for treatment in this document, although frequently stated as medical diagnosis, are merely
provider impressions to guide the EMS care provider in initiating appropriate treatment. This document is to be used as
consultative material in striving for optimal patient care. It is recognized that specific procedures or treatments may be
modified depending on the circumstances of a particular case. A medical control physician should be contacted anytime there
is a concern regarding the patient’s status.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1125
CISD AND PEER COUNSELING
1125 - CISD AND PEER COUNSELING
EMS personnel are encouraged to familiarize themselves with the causes and contributing factors of critical incident and cumulative
stress, and learn to recognize the normal stress reactions that can develop from providing emergency medical services. An EMS Peer
Counseling Program is available to EMS personnel through the Regional EMS Programs. The program consists of mental health
professionals, chaplains, and trained peer support personnel who develop stress reduction activities, provide training, conduct
debriefings, and assist EMS personnel in locating available resources. The team will provide voluntary and confidential assistance
to those wanting to discuss conflicts or feelings concerning their work or how their work affects their personal lives.
A critical incident is any response that causes EMS personnel to experience unusually strong emotional involvement. A formal or
informal debriefing will be provided at the request of medical authorities, ambulance management or EMS personnel directly related
to the incident.
Contact information for Regional EMS Programs is available on the EMSRB website at
www.emsrb.state.mn.us or call 612-207-1130 to contact a Metro CISM Team.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1150
DEAD ON ARRIVAL (DOA)
1150 - DEAD ON ARRIVAL (DOA)
DOA Criteria Defined:
A pulseless, apneic patient can be called deceased on arrival if the following signs are present:
Rigor mortis (Caution: do not confuse with stiffness due to cold environment.)
Dependent lividity.
Decomposition.
Decapitation.
Severe trauma that is not compatible with life.
Incineration.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1175
DNR AND LIVING WILLS
1175 - DNR AND LIVING WILLS
Do Not Resuscitate (DNR, RPOLST) orders are orders issued by a patient’s physician to refrain from initiating resuscitative measures
in the event of cardiopulmonary arrest. Patients with DNR orders should receive vigorous medical support, including all interventions
specified in the Medical Protocols, up until the point of cardiopulmonary arrest.
In the nursing home, a DNR order is valid if it is written in the order section of the patient chart (or on a transfer form)
and is signed by a physician, registered nurse practitioner, or physician assistant acting under physician authority. Copies of
the order are valid. In a private home, the standard DNR or POLST form must be signed by the patient or proxy, the physician, and
a witness in order to be valid. No validation stamp or notarization is necessary, and a legible copy is acceptable.
If possible, the DNR / POLST order or copy should accompany the patient to the hospital. Pertinent documentation should be included
on the ambulance report form for the run. In the event of confusion or questions regarding the DNR / POLST order, resuscitation
should be initiated and a medical control physician should be consulted.
Living Wills The presence of a living will should not alter your care. The living will cannot be interpreted in the
field. Living wills should not be interpreted at the scene but conveyed to the physicians in the receiving Emergency Department.
DNR (Do Not Resuscitate)
CPR may be withheld if apneic, pulseless (at-home) patient has a Minnesota Medical Association DNR or POLST
Form signed by themselves or their guardian, a witness and their physician. MUST be signed by all
three.
CPR may be withheld if apneic, pulseless nursing home patient has an order in their medical record signed by their
physician. This order (does not need to be the formal DNR Form)
When the patient is NOT apneic and pulseless, standard medical care should be provided regardless of their DNR
status.
The only Valid HOME DNR Order is a Minnesota Medical Association DNR (or POLST) Form or EMSRB DNR
Form signed by the patient or their legal guardian, a witness and their physician. All three signatures MUST be present.
Copies are valid. No validation stamp or notarization is necessary. A VALID Nursing Home DNR Order is a signed physician
order that can be found in the patient’s medical chart.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1200
INFECTION CONTROL PLAN
1200 - INFECTION CONTROL PLAN
Minnesota Statute 144E.125 Operation Procedures, requires that Minnesota Licensed Ambulance Services have a procedure for
infection control.
Ambulance Services are required to comply with OSHA regulation 1910.1030(c)
Universal precautions (aka - Standard precautions) refers to the practice, in medicine, of avoiding contact with patient’s
bodily fluids, by means of the wearing of nonporous articles such as medical gloves, goggles, and face shields. Medical instruments
should be handled carefully and disposed of properly in a sharps container. Pathogens fall into two broad categories, blood borne
(carried in the body fluids) and airborne. Universal precautions cover both types.
Universal precautions should be practived in any environment where workers are exposed to body fluids, such as:
Blood
Sputum
Semen
Vaginal secretions
Synovial fluid
Amniotic fluid
Cerebrospinal fluid
Pleural fluid
Peritoneal fluid
Pericardial fluid
Whenever providing care for a patient with a febrile respiratory illness, perform the following:
Wear a mask
Wear eye protection if productive cough present and while performing any procedure which may result in droplet production
(nebs)
What is a “Significant Exposure”?
Patient’s blood or body fluids contact an opening in the skin (e.g. cuts, abrasions, dermatitis or blisters) or if there
is prolonged contact or an extensive area is exposed.
Blood or body fluids sprayed into your eyes, nose or mouth.
Puncture wound from a needle, human bites, or other sharp object that has had contact with the patient’s blood or body
fluids.
Potential exposure or known exposure to airborne transmitted organisms (e.g. Tuberculosis) or droplet transmitted organism
(e.g. Meningitis).
How do I prevent a "Significant Exposure"?
Use gloves for patient contact, shielded face masks and/or mask with safety goggles for airway management, shielded masks
with gowns for obstetrical deliveries, N-95 masks for potential TB patients or patients coughing bloody sputum and/or
experiencing night sweats with weight loss.
What if a "Significant Exposure" occurs?
Wash the exposed skin, blow your nose, irrigate your eyes, and consider gargling as soon as possible.
Report the incident immediately to your supervisor.
Follow the infectious source (patient) to the hospital for a post exposure evaluation.
Report to the ER to initiate Exposure protocol.
For additional information, see Ridgeview Procedure P10300 - Ambulance Infection Control Procedures
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1225
MANDATORY REPORTING ISSUES
1225 - MANDATORY REPORTING ISSUES
It is mandatory to report certain crimes, failure to report these incidents may be a crime itself. Minnesota offers immunity from
liability for people who report incidents in good faith. When required to report these incidents you are exempt from patient
confidentiality requirements.
Minnesota State statute (626.556-67) requires the EMT to report the following:
You must document clearly on the patient care report that your concerns have been reported to the receiving facility.
Discuss your concerns with the service if you have any question about the requirement to report an incident.
EMSRB Mandatory Reporting Requirements
Ambulance Services are mandated to report to the Minnesota EMS Regulatory Board in compliance with the following statutes:
MINNESOTA STATUTE 144E.305 - REPORTING MISCONDUCT
Subd. 2. Mandatory reporting. (a) A licensee shall report to the board conduct by an emergency medical responder,
EMT, AEMT, or paramedic that they reasonably believe constitutes grounds for disciplinary action under section 144E.27,
subdivision 5, or 144E.28, subdivision 5. The licensee shall report to the board within 60 days of obtaining verifiable
knowledge of the conduct constituting grounds for disciplinary action.
(b) A licensee shall report to the board any dismissal from employment of an emergency medical responder, EMT, AEMT, or
paramedic. A licensee shall report the resignation of an emergency medical responder, EMT, AEMT, or paramedic before the
conclusion of any disciplinary proceeding or before commencement of formal charges but after the emergency medical responder,
EMT, AEMT, or paramedic has knowledge that formal charges are contemplated or in preparation. The licensee shall report to the
board within 60 days of the resignation or initial determination to dismiss. An individual's exercise of rights under a
collective bargaining agreement does not extend the licensee's time period for reporting under this subdivision.
Purpose
The purpose of this document is to outline and educate BLS Ambulance Services concerning the policies and procedures
needed to comply with the patient privacy rights enacted under the Health Insurance Portability and Accountability
Act of 1996 (HIPAA).
Policy
The patient has the right to receive a privacy notice in a timely manner. Upon request, the patient may at
any time receive a paper copy of the privacy notice, even if he or she earlier agreed to receive the notice
electronically.
Requesting restrictions on certain uses and disclosures. The patient has the right to object to, and
ask for restrictions on, how his or her health information is used or to whom the information is disclosed,
even if the restriction affects the patient’s treatment, payment, or health care operation activities. The
patient may want to limit the health information that is included in patient directories, or provided to family
or friends involved in his or her care or payment of medical bills. The patient may also want to limit the
health information provided to authorities involved with disaster relief efforts. However, we are not required
to agree in all circumstances to the patient’s requested restriction.
Receiving confidential communication of health information. The patient has the right to ask that we
communicate his or her health information to them in different ways or places. For example, the patient may
wish to receive information about their health status in a special, private room or through a written letter
sent to a private address. We must accommodate requests that are reasonable in terms of administrative burden.
We may not require the patient to give a reason for the request.
Access, inspection and copying of health information. With a few exceptions, patients have the right to
inspect and obtain a copy of their health information. However, this right does not apply to psychotherapy notes
or information gathered for judicial proceedings, for example. In addition, we may charge the patient a reasonable
fee for copies of their health information.
Requesting amendments or corrections to health information. If the patient believes their health information
is incomplete or incorrect, they may ask us to correct the information. The patient may be asked to make such
requests in writing and to give a reason as to why his or her health information should be changed. However, if we
did not create the health information that the patient believes is incorrect, or if we disagree with the patient
and believe his or her health information is correct, we may deny the request. We must act on the request within
60 days after we receive it, unless we inform the patient of our need for a one-time 30-day extension.
Receiving an accounting of disclosures of health information. In some limited instances, the patient has the
right to ask for a list of the disclosures of their health information that we have made during the previous six
years, but the request cannot include dates before April 14, 2003. This list must include the date of each disclosure,
who received the disclosed health information, a brief description of the health information disclosed, and why the
disclosure was made. We must furnish the patient with a list within 60 days of the request, unless we inform the
patient of our need for a one-time 30-day extension, and we may not charge the patient for the list, unless the patient
requests such list more than once in a 12 month period. In addition, we will not include in the list disclosures made
to the patient, or for purposes of treatment, payment, health care operations, national security, law enforcement/corrections,
and certain health oversight activities.
Complaints. Patients have the right to file a complaint with an ambulance service and with the federal Department of
Health and Human Services if they believe their privacy rights have been violated. We will not retaliate against the patient
for filing such a complaint.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1275
PATIENT CONSENT AND REFUSAL OF CARE
1275 - PATIENT CONSENT AND REFUSAL OF CARE
See RMC Procedure/Guideline #P10048
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1300
PHYSICIAN OR MEDICAL PROVIDER ON SCENE
1300 - PHYSICIAN OR MEDICAL PROVIDER ON SCENE
If a Physician / Registered Nurse / Physician Assistant is present on scene, and wishes to to assume medical direction, the
following must occure:
Provider must:
Produce identification and copy of a Valid Minnesota Medical License.
Agree to accompany the patient to the receiving facility.
Agree to sign the patient care report assuming medical responsibility for the patient.
Medical Control must be informed and consent to the provider assuming on scene medical direction.
If the physician does accept the terms above, upon arrival at the hospital obtain a photo copy of the
license and attach to the patient care report.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1325
RESPONSE OBLIGATIONS
1325 - RESPONSE OBLIGATIONS
Obligated to Assess and Treat
When you respond to an emergency medical call, you are obligated to assess and treat the patient. Responsibility for
the patient continues until a higher medical authority (paramedic, registered nurse, PA, nurse practitioner and/or
physician) assumes care.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
General Administration Guideline
Guideline Number - 1400
RESTRAINT USE
1400 - RESTRAINT USE
To provide guidance and criteria for the use of physical restraint of patients during care and transport.
Any mechanism used to physically confine a patient. This includes, but is not limited to: soft composite dressing, tape,
leathers or hand cuffs wrapped and secured at the wrist and/or ankles and/or chest or lower extremities.
If EMS personnel judge it necessary to restrain a patient to protect him/her self from injury, or to protect others
(bystanders or EMS personnel) from injury:
Document the events leading up to the need for restraint use in the patient record.
Document the method of restraint and the position of restraint in the patient record.
Document the reason for restraining the patient.
In the event that the patient spits, the rescuer may place over the patient’s mouth and nose a surgical mask or an
oxygen mask that is connected to high flow oxygen.
Inform patient of the reason for restraint.
Restrain patients in a manner that does not impair circulation or cause choking or aspiration. DO NOT restrain
patients in the prone position (face down). Prone restraint has the potential to impair the patient’s ability to breathe
adequately. Police officers are trained in restraining violent individuals safely. Utilize the police on the scene in deciding
the appropriate restraint technique to maximize the safety of the rescuers and the patient.
As soon as possible, attempt to remove any potentially dangerous items (belts, shoes, sharp objects, weapons) prior to restraint.
Any weapons or contraband (drugs, drug paraphernalia) shall be turned over to a Law Enforcement Officer.
Assess the patient’s circulation (checking pulses in the feet and wrists) every 15 minutes while the patient is
restrained. If circulation is impaired, adjust or loosen restraints as needed. Document the presence of pulses in each extremity and
the patient’s ability to breathe after restraint is accomplished. Be prepared to turn the patient to facilitate clearance of the
airway while also having suction devices readily available.
Inform hospital personnel who assume responsibility for the patient’s care at the hospital of the reason for restraining the
patient.
The EMT at his discretion may request that law enforcement accompany and or follow the patient to the hospital. Any patient
restrained in handcuffs shall have law enforcement accompany the patient in the patient compartment or follow the ambulance
.
Airway and breathing problems are the most common cause of cardiac arrest in children.
Do not hyperextend the neck when opening the airway in newborns or infants.
Use a Bag-Valve-Mask (BVM) or mouth to mask with one-way valve with supplemental oxygen to ventilate a child.
0 yr. to 5 yr. - 400cc BVM (infant size)
5 yr. to 90lbs. – 1000cc BVM (child size)
Newborns and infants are more prone to becoming hypothermic (cold). Prevent heat loss.
VITALS Sign Reference
Trauma Considerations
AIRWAY
Airway remains the top priority while maintaining spinal precautions:
Establish and maintain an open airway using the modified jaw thrust.
All unconscious patients require an oral or nasal airway.
Begin oxygen therapy as soon as possible.
If the patient vomits or has fluids in airway: MAINTAIN SPINAL STABILIZATION AND LOG ROLL PATIENT TO SIDE AS A UNIT to
clear out or suction the airway.
SPINAL PRECAUTIONS (manual head stabilization and rigid cervical collar. Use spine board only if needed for extrication
or movement)
Take spinal precautions whenever a trauma patient has:
Experienced a mechanism of injury that could cause an injury to the spine.
Loss of consciousness or altered level of consciousness.
Any complaint of numbness, tingling or inability to move extremities.
Complaints of pain in the head, neck, or back.
Evidence of intoxication or under the influence of drugs.
Head and/or facial trauma.
Penetrating injury to the head, neck or trunk.
Ambulatory patients with normal mental status and no neck/back pain or spine tenderness, do not require
immobilization.
NOTE: If in doubt immobilize.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
BLS Protocols
2020
ANAPHYLAXIS
2020 - ANAPHYLAXIS
Care Goals:
Provide timely therapy for potentially life-threatening reactions to known or suspected allergens
Assessment:
Assess airway, check for swelling or redness in oropharynx
Assess respiratory effort, auscultate lungs for wheezing or crackles
Assess perfusion: Skin signs, cap refill, mental status
Assess for Anaphylaxis
Severe, rapid symptom onset involving skin and/or mucosa with respiratory compromise and/or hypotension in a patient
after exposure to a known allergen.
OR
Two or more of the following occurring rapidly after exposure to a likely allergen:
Skin and/or mucosal involvement (hives, itching, swollen tongue/lips) CAUTION: Skin involvement may be ABSENT in up to 40%
of cases
Hypotension or associated symptoms (syncope, weakness, chest tightness, incontinence)
Management:
Follow appropriate pathway based on findings and criteria above:
Mild, Non-Anaphylactic Allergic Reactions
Begin transport
Consider ALS intercept
If transportation to destination would be quicker than ALS intercept, or destination is in opposite direction than ALS
intercept, crew can forgo ALS intercept
Anaphylaxis (criteria are above)
Administer 1 Adult EpiPen IM.
May repeat as needed every five to ten minutes.
If supply of adult EpiPens is exhausted, may substitute pediatric EpiPen.
Manage airway as appropriate
Begin emergent transport
Consider ALS intercept
If transportation to destination would be quicker than ALS intercept, or destination is in opposite direction than ALS
intercept, crew can forgo ALS intercept
If varianced, establish IV during transport
If bronchospasm and/or wheezing exists after administration of Epinephrine:
Nebulized medications (may nebulize continuously without improvement):
Protect patient from complications of altered mental status (e.g., respiratory failure, shock, cardiopulmonary arrest)
Care Goals:
Look for treatable causes of altered mental status (AMS):
Airway: Make sure airway remains patent; reposition patient as needed
Breathing: Look for respiratory depression. Check SPO2 and CO detector readings if applicable
Circulation: Look for signs of poor perfusion
Glasgow Coma Score and/or AVPU
Pupils
Head and neck: Evaluate for signs of trauma
Neck: Rigidity or pain with range of motion
Stroke assessment tool including focal neurologic findings
Blood glucose level
Breath odor: Alcohol, Acidosis, Ammonia
Chest/Abdominal: Intra-thoracic hardware, assist devices, abdominal pain or distention, signs of trauma
Extremities/skin: Track marks, hydration, edema, dialysis shunt, temperature to touch (or if able, use a thermometer), signs of
trauma
Signs of infection: Fever, Cough, skin changes, dysuria
Environment: Survey for pills, paraphernalia, substance use, medication patches, medical devices, ambient temperature, social
indicators of neglect, carbon monoxide exposures, multiple casualties with same complaint
Management:
With depressed mental status, initial focus is on airway protection, oxygenation, ventilation, and perfusion
The violent patient may need pharmacologic and/or physical management to ensure proper assessment and treatment
If transportation to destination would be quicker than ALS intercept, or destination is in opposite direction than ALS
intercept, crew can forgo ALS intercept
Patient IS breathing
Severe
Consider manual exhalation
Administer medications as indicated:
Nebulized medications (may repeat continuously without improvement):
If transportation to destination would be quicker than ALS intercept, or destination is in opposite direction
than ALS intercept, crew can forgo ALS intercept
Mild to Moderate
Consider manual exhalation
Administer medications as indicated:
Nebulized medications (may repeat continuously without improvement):
If transportation to destination would be quicker than ALS intercept, or destination is in opposite direction
than ALS intercept, crew can forgo ALS intercept
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2100
BEHAVIORAL OR PHYCHIATRIC EMERGENCIES
2100 - BEHAVIORAL OR PHYCHIATRIC EMERGENCIES
Ensuring the safety of EMS personnel is of paramount importance. Always summon law enforcement to secure the scene
and patient before attempting to provide medical care. Be aware of items at the scene or medical equipment that may become
a weapon.
Care Goals:
Provision of emergency medical care to the agitated, violent, or uncooperative patient
Maximizing and maintaining safety for EMS personnel, patient, and others
Assessment:
Obtain history from family, friends, witnesses, or patient if possible
Conduct as thorough a physical examination as can be done under the circumstances
Note medications/substances on scene that may contribute or be relevant to the agitation
Note respiratory rate and effort – if possible, monitor pulse oximetry
Assess circulatory status
Assess for evidence of traumatic injuries
Assess mental status
Assess for hyperthermia (tactile temp)
Check blood sugar and temperature if safe to do so
Management:
Guidelines for the Management of Uncooperative, Agitated, Violent, or Potentially Violent Patients Secondary to a
Medical Disorder
Assure appropriate police agency has been notified.
Obtain history from family, friends, witnesses or patient if possible.
Conduct as thorough a physical examination as can be done under the circumstances.
Keep calm. Do not get angry with the patient. Talk slowly and clearly; do not shout or threaten. Constantly reassure the patient
and constantly keep the patient informed of what you are doing and why.
If the patient becomes violent, or his actions present a threat to his safety or that of others, immediate restraint may be
necessary.
Guidelines for the Management of an Obviously Mentally Ill Person Who Is Violent or Considered to be Potentially Violent (Primary
Mental Heatlh Concern):
If physical violence has occurred or there is likelihood that the patient has access to a weapon, do not intervene. Take precautions
for your own safety and that of others at the scene. Call for police assistance and await their arrival.
If no violence has occurred and the patient does not have access to weapons and can be approached with minimal danger to EMS
personnel:
Attempt to calm the patient.
Do not shout or threaten.
Identify yourself. Speak slowly, clearly and remain in control of your emotions.
Explain why you are there and that you would like to help him/her.
If patient continues to present a risk of violence, becomes increasingly agitated and uncooperative, do not force the issue.
Withdraw and wait for law enforcement personnel.
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2125
CARDIAC ARREST
2125 - CARDIAC ARREST
Care Goals:
Return of spontaneous circulation (ROSC)
Preservation of neurologic function
High-quality chest compressions/CPR with minimal interruption from recognition of cardiac arrest until confirmation
of ROSC or field termination of care
Assessment:
The patient in cardiac arrest requires a prompt balance of treatment and assessment
In cases of cardiac arrest, assessments should be focused and limited to obtaining enough information to reveal the patient is
pulseless
Once pulselessness is discovered, treatment should be initiated immediately, and any further history must be obtained by bystanders
while treatment is ongoing
Management:
Immediately start Basic Life Support (BLS):
Begin CPR using 30:2 Compression:Ventilation Ratio at a rate of 100-120 compressions/min
Attach AED and follow prompts for pulse checks and defibrillation
If defibrillation indicated, deliver shock
Immediately resume CPR
Attach Impedance Threshold Device (ITD, ResQPod) to BVM
Apply to patient within 30 seconds. You must maintain a tight, continuous, 2-handed face mask seal for the ITD to
function properly
Place patient in Lucas Device when able
After patient receives defibrillation x1 without ROSC, activate Refractory V-fib/ Mobile ECMO if patient meets criteria (see
below item 5 below) and expedite transport
Destinations include:
ALS intercept
Helicopter LZ for ecmo candidates
Closest hospital.
Place an advanced airway (iGel or other BLS advanced airway) - while continuing compressions with inline ETCO2
Once advanced airway has been placed, ventilate at 10 breaths/min timed on compression upstroke
If poor ETCO2 waveform, decreasing SpO2 or poor chest rise consider switching back to 30:2
Obtain IV/IO access while providing CPR (if authorized).
If patient has received at least 3 defibrillations and the above interventions have been unsuccessful in achieving ROSC, perform
vector-change defibrillation, using the following guidelines:
If pad position for initial defibrillation attempts was Anterior-Lateral, position a new set of pads in Anterior-Posterior
positioning.
If pad position for initial defibrillation attempts was Anterior-Posterior, position a new set of pads in Anterior-Lateral
positioning
Refractory V-Fib/ Mobile ECMO Activation (BLS only Tier 2 locations):
For patients who have received 1 defibrillation attempt (including from AED prior to EMS arrival) without ROSC and who meet inclusion
criteria below – contact W-MRCC as soon as possible (which may be prior to EMS arrival) to activate mobile ECMO, ensure Life Link III
is started and expedite transport to designated landing zone
Inclusion criteria (if not met, continue to provide cardiac arrest care per protocol above):
Age 18-75
Shock Indicated by AED on first rhythm check
Total CPR time expected to be < 60 minutes prior to ECMO flow
Chest size able to fit in LUCAS CPR device
Independently living
Arrest is presumed to be of cardiac etiology
Ensure Life Link III helicopter has been started
Provide EARLY communication to destination with patient info (age, gender, pertinent clinical findings/ medical history, ETA)
For ecmo candidates use Verbiage “Red patient, Mobile ECMO activation” when hailing W-MRCC
Standby by tac channel assignment and communication with ECMO physician as needed.
If inclusion criteria are met, prioritize limiting scene time/ loading and transporting as quickly/ safely as possible:
Ensure First Responder help (two) and extra batteries for transport
Continue cardiac arrest management
Place patient on LUCAS CPR device
Place iGel
Obtain IV/IO access (if authorized)
Changes in condition (e.g. ROSC, PEA, asystole, etc.) should not change destination once activated
Contact W-MRCC or call 612-638-4901 if you wish to speak directly with a mobile ECMO physician
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2150
CARE OF THE NEWBORN
2150 - CARE OF THE NEWBORN
Care Goals:
Plan for resources based on number of anticipated patients (e.g., mother and newborn or multiple births)
Provide routine care to the newly born infant
Perform a neonatal assessment
Rapidly identify newly born infants requiring resuscitative efforts
Provide appropriate interventions to minimize distress in the newly born infant
Recognize the need for additional resources based on patient conditions and/or environmental factors
Assessment and Early Management:
In all situations including during assessment, minimize the newborn’s heat loss:
Dry the newborn well.
Increase environmental temperature
Suction the newborn only if needed to clear secretions
Assess for apnea, gasping, or heart rate less than 100:
If apneic, gasping, or heart rate less than 100, initiate positive pressure ventilation, monitor SpO2.
If labored breathing or persistent cyanosis, reposition airway and administer oxygen (less than 30% FiO2).
Reassess heart rate:
If less than 100: correct ventilation or increase oxygen.
If less than 60: start chest compressions, increase oxygen to 100%, and place iGel
Continue to reassess heart rate
Gather history:
Date and time of birth
Onset of labor
Prenatal history (prenatal care, substance abuse, multiple gestation, maternal illness)
Birth history (maternal fever, presence of meconium, maternal bleeding, difficult delivery (e.g., shoulder dystocia, prolapsed
or nuchal cord, breech))
Estimated gestational age (may be based on last menstrual period)
Physical examination:
Respiratory rate and effort (strong, weak, absent, or irregular)
Signs of respiratory distress (grunting, nasal flaring, retractions, gasping, apnea)
Heart rate
Direct palpation of chest wall, umbilical stump, or brachial pulse may be used (chest auscultation is preferable due to its
accuracy)
If immediate resuscitation is required and the newborn is still attached to the mother, clamp the cord in two places and cut between the
clamps 8-10 inches from infant. If no resuscitation is required, warm/dry/stimulate the newborn, and then cut/clamp the cord after 60
seconds or the cord stops pulsating
After performing the above assessments and interventions (if indicated):
If no need for immediate resuscitation, wait 30-60 seconds then double clamp and cut the umbilical cord approximately 8-10 inches
from the infant.
Term infants (> 37weeks) who are crying (good respiratory effort) and have good muscle tone can be given to the mother to nurse
with continued warming efforts and re- assessment.
Transport; do not wait for nor attempt delivery of the placenta.
Closely observe the infant for signs and symptoms of distress and monitor the mother for excessive postpartum bleeding.
Considerations:
Approximately 10% of newly born infants require some assistance to begin breathing at birth and 1% require resuscitation to support
perfusion
Most newborns require only drying, warming, and stimulating to help them transition from fetal respiration to newborn
respiration.
The resuscitation sequence can be remembered as Dry, Warm, and Stimulate – Ventilate – Evaluate – and Resuscitate.
Deliveries complicated by maternal bleeding (placenta previa, vas previa, or placental abruption) place the infant at risk for
hypovolemia secondary to blood loss
Low birth weight infants are at high-risk for hypothermia due to heat loss and a higher surface area to volume ratio.
Measuring the pulse oximetry on the right hand provides the most accurate oxygen saturation (SpO2) in infants that are
transitioning from fetal to normal circulation.
At 60 seconds, 60% is the target with an increase of 5% every minute until 5 minutes of life when pulse oximetry is 80–85%
Both hypoxia and excess oxygen administration can result in harm to the infant. If prolonged oxygen use is required, titrate to maintain
an SpO2 of 85–95%
While not ideal, a larger facemask than indicated for patient size may be used to provide BVM ventilation if an appropriately sized mask
is not available.
Avoid pressure over the eyes as this may result in bradycardia
A multiple gestation delivery may require additional resources and/or clinicians.
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2200
CHEST PAIN/DISCOMFORT (SUSPECTED MI)
2200 - CHEST PAIN/DISCOMFORT (SUSPECTED MI)
Care Goals:
Identify Acute Coronary Syndrome quickly
Determine time of symptom onset
Activate hospital-based systems of care
Monitor vital signs and be prepared to provide CPR and defibrillation if needed
Administer appropriate medications
Transport to appropriate facility
Assessment:
Assess respiratory status, especially dyspnea, hypoxia, or signs of heart failure including pulmonary edema, JVD, pedal edema.
Assess for signs and symptoms of Acute Coronary Syndrome:
Chest pain or discomfort in other areas of the body (e.g., arm, jaw, epigastrium) of suspected cardiac origin
Shortness of breath, associated or unexplained sweating, nausea, vomiting, or dizziness.
Atypical or unusual symptoms are more common in women, the elderly, and diabetic patients.
May also present with CHF, syncope, and/or shock
Patients with a history of MI should be asked to compare their current complaint to their prior MI(s)
Chest pain associated sympathomimetic use (e.g., cocaine, methamphetamine)
Some patients will present with likely non-cardiac chest pain and otherwise have a low likelihood of ACS (e.g., blunt trauma to the
chest of a child). For these patients, defer the administration of aspirin (ASA) and nitrates
If available, perform 12 lead and evaluate heart rate
Management:
Administer supplemental oxygen only if SpO2 < 93%
If the patient is severely dyspneic, hypoxemic, or has obvious signs of heart failure, EMS clinicians should administer oxygen as
appropriate with a target of achieving 94–98% saturation
Place AED Pads on patients who present with or develop signs of clinical deterioration:
Worsening chest pain, shortness of breath, decreased level of consciousness/syncope, or other signs of shock/hypotension
Administer aspirin (ASA) - 324mg by mouth if the patient has no history of allergy.
Administer nitroglycerin lingual spray - 0.4 mg metered dose spray if the patient's systolic BP is greater than or equal to 100.
Consult with medical control physician if systolic BP is less than 100.
Check the BP immediately prior to and after administration of nitro. Care should always be taken when giving nitroglycerin
when the patient’s blood pressure is marginal.
Repeat every 5 min for continued pain
The use of nitrates should be avoided in any patient who has used a phosphodiesterase inhibitor within the past 48 hours. CAUTION:
In addition to their use for erectile dysfunction, these medications may be used for pulmonary hypertension, including in females.
Examples include:
sildenafil (Viagra®, Revatio®)
vardenafil (Levitra®, Staxyn®)
tadalafil (Cialis®, Adcirca®)
Also avoid use in patients receiving intravenous epoprostenol (Flolan®) or treporstenil (Remodulin®) which are used for
pulmonary hypertension
Obtain IV access (if authorized)
Obtain 12-lead ECG (if authorized)
Transport and destination decisions should be based on local resources and system of care
A complete medication list should be obtained from each patient. It is especially important for the treating physician and healthcare
providers to be informed if the patient is taking beta-blockers, calcium channel blockers, clonidine, digoxin, blood thinners
(anticoagulants), and medications for the treatment of erectile dysfunction or pulmonary hypertension
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2225
CHF/PULMONARY EDEMA
2225 - CHF/PULMONARY EDEMA
Care Goals:
Assure adequate oxygen and ventilation
Recognize impending respiratory failure
Promptly identfiy and intervene for patients who require escalation of therapy
Deliver appropriate therapy by differentiating likely cause of respiratory distress
Keep the patient’s head elevated, raise head on stretcher fully
Begin oxygen therapy:
Supplemental oxygen for dyspnea to a target 94-98% SpO2
If the patient’s respiratory distress is severe, consider positive pressure ventilatory assistance if the patient is able to
tolerate.
Give nitroglycerin lingual spray - 0.4 mg metered dose spray SL x 2 if the patient’s systolic BP is 140 or greater.
Two minutes after the initial nitro dose, repeat nitroglycerin 0.4 mg metered dose spray SL x 1 if the patient still has signs of
pulmonary edema AND the systolic BP remains 140 or greater.
Five minutes after the second dose, repeat nitroglycerin 0.4 mg metered dose spray SL x 1 if the patient still has signs of pulmonary
edema and the systolic BP is 140 or greater.
The use of nitrates should be avoided in any patient who has used a phosphodiesterase inhibitor within the past 48 hours. CAUTION:
In addition to their use for erectile dysfunction, these medications may be used for pulmonary hypertension, including in females.
This is especially true of patients presenting with pulmonary edema, since it can be caused by pulmonary hypertension. Examples
include:
sildenafil (Viagra®, Revatio®)
vardenafil (Levitra®, Staxyn®)
tadalafil (Cialis®, Adcirca®)
Also avoid use in patients receiving intravenous epoprostenol (Flolan®) or treporstenil (Remodulin®) which are used for
pulmonary hypertension
Give aspirin (ASA) -324mg by mouth if the patient has no history of allergy.
If the patient has no relief and their systolic BP remains 140 or greater:
Repeat nitroglycerin every three to five minutes as necessary. Recheck the patient’s BP before and after administration
Consider CPAP if two or more of the following are present:
Retractions or accessory muscle use.
Pulmonary edema.
Respiratory rate greater than 25/min.
SpO2 less than 92%.
If indicated, Administer CPAP (CPAP MODE) to achieve 11 - 12 cm H2O (15 LPM).
CAUTION: CPAP can cause rapid hypotension. Set monitor to take pressures every 5 minutes.
Assess the patient’s response. If the patient’s condition worsens, (e.g. the patient becomes hypotensive, decreased SpO2)
discontinue CPAP.
If CPAP is initiated, continue to treat with medications as normal.
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2250
CVA/STROKE
2250 - CVA/STROKE
Care Goals:
Detect neurological deficits
Identify candidates for Stroke Alert
Determine eligibility for transport to a stroke center
Facilitate appropriate downstream care for neurological emergencies
Perform B.E.F.A.S.T Stroke Scale (includes: Balance, Eyes/vision, Facial droop, Arm drift, Speech and Time)
Balance: sudden loss of balance or coordination, SUSTAINED vertigo or vertigo with other focal symptoms.
Eye: Bilateral visual field cut or double vision
Facial droop or weakness
Arm pronator drift or leg weakness
Speech difficulties, slurred speech, or aphasia (unable to repeat, name or follow simple commands)
Thunderclap headache
Determine possible LVO (Large Vessel Occlusion)
Arm drift PLUS
Visual field cut OR
Aphasia OR
Neglect (forced lateral gaze or ignoring one side)
If B.E.F.A.S.T Stroke Scale is positive (abnormal findings)
If within 24 hours of symptom onset OR last known well:
Expedite Transport
Use “STROKE CODE” in radio report, and
Give time of symptom onset OR last known well in clock time (e.g. 2:30pm)
If positive but known to be more than 24 since symptom onset:
Don’t use “STROKE CODE” in radio report, but do state time of symptom onset in radio report
If time of symptom onset is unknown (e.g. patient is unable to communicate), then:
Expedite Transport
Use “STROKE CODE” in radio report, and state “unknown symptom onset time” in radio report
Document last known well time on your PCR
Assess for other related factors:
History of Atrial Fibrillation
Taking warfarin or any anticoagulant medication
History of recent
Trauma
Travel
Seizure
Surgery
Hemorrhage (e.g., GI bleed)
Evaluate for the presence of stroke mimics including:
Hypoglycemia
Seizure
Sepsis
Migraine
Intoxication
Management:
If a “STROKE CODE” is indicated by the above criteria, the main priority is getting the patient safely to an appropriate facility
in a timely fashion
Prevent aspiration – elevate head of stretcher 15–30 degrees if systolic BP greater than 100 mmHg
Maintain head and neck in neutral alignment, without flexing the neck
Protect paralyzed limbs from injury
Avoid multiple IV attempts, and do not attempt IV on scene
If applicable, bring a family member or other witness or person familiar with the patient’s normal mental status.
Monitor closely for new or worsening neurological exam findings during transport such as:
Facial droop
Localized Weakness
Ataxic or uncoordinated movements
Slurred speech
Altered Mentation
Sudden onset of dizziness/vertigo
Hemiparesis or hemiplegia
Dysconjugate, forced, or crossed gaze
Severe headache, neck pain/stiffness, difficulty seeing
Be aware that an outwardly stable stroke patient may rapidly decline in your care.
Transport to facility of pt choice unless:
Possible LVO: Direct to Comprehensive (Abbott, HCMC, U of MN, North, Methodist, Regions, United) or Primary -Thrombectomy
capable (Southdale, Mercy) Stroke center.
Closer hospital if patient requested hospital (or LVO destination) adds more than 30 minutes or the total transport time
would be more than 45 min.
Closest hospital if approaching 4 hrs since onset or last known well to stay within the 4.5 hr cut off for possible
thrombolytic therapy (including LVO patients).
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2275
DIABETIC EMERGENCIES
2275 - DIABETIC EMERGENCIES
Care Goals:
Limit morbidity and mortality from abnormal blood glucose levels
Treat symptomatic hypoglycemia
Tailor patient education and disposition to prevent recurrence
If above treatment does not achieve normal blood sugar and mental status:
Initiate transport
Evaluate for alternative causes of mental status, evaluate per 2250 - CVA / Stroke
Continue ongoing treatment as feasible
AFTER OBTAINING VERBAL ORDERS:
In general, EMS should transport all patients on oral hypoglycemic agents or long-acting insulin.
All hypoglycemic patients who had a seizure should be transported to the hospital regardless of their mental status and response
to therapy
If symptoms resolve after treatment, release without transport is should only be considered if ALL of the following are true:
Repeat glucose greater than 80 mg/dL
Patient takes insulin or metformin to control diabetes and does not take long-acting oral sulphonylurea agents
Patient returns to normal mental status, with no focal neurologic signs/symptoms after receiving glucose/dextrose
Patient can promptly obtain and will eat a carbohydrate meal
Patient or legal guardian refuses transport and EMS clinicians agree transport not indicated
A reliable adult will be staying with patient
No major co-morbid symptoms exist such as chest pain, shortness of breath, seizures, intoxication
A clear cause of the hypoglycemia is identified (e.g., missed meal)
Considerations There are several classes of medications used for diabetes. Patients may be on one or several different
medications for their diabetes. In general, insulin and sulfonylurea medications are the highest risk for
causing hypoglycemia on their own. However, the effects of all these medications can be additive, meaning
a lower risk drug can still cause ongoing or rebound hypoglycemia. Consider these factors when treating or
determining a disposition for a hypoglycemic patient.
Insulins: Injectable medications, act directly to allow glucose uptake by cells. HIGH RISK OF CAUSING HYPOGLYCEMIA
Long Acting Insulin, 24 hour duration. Usually, but not always found as a pen
Lantus (Insulin Glargine)
Detemire (Insulin Levemire)
Intermediate Acting Insulin, Peak at 4-10 hours. Usually found in a vial
Humulin R, Novolin R (Insulin NPH)
Short Acting Insulin, Peak at 2-4 hours. Usually found in a vial
Humulin N, Novolin N (Regular Insulin)
Rapid Acting Insulin. Peak at 1-2 hours. May be found as a pen or in a vial
Humalog (Insulin Lispro)
Novolog (Insulin Aspart)
Apidra (Insulin Glulisine)
Metformin (Glucophage): Oral medications. Reduces glucose output from liver, decreases insulin resistance. When used alone, Metformin
has a lower risk of hypoglycemia, however it is HIGH RISK when combined with other medications, especially insulin and
sulfonylureas
Incretin Mimetics “Tides”: Injectable medications. Increase insulin output from pancreas, decrease glucose output from liver, slows
sugar uptake from digestion, decreases appetite, increases effect of insulin. considered lower risk on its own, can become HIGH RISK
when combined with other medications, especially insulin and sulfonylureas
Exenatide (Byetta)
Exenatide LAR (Bydureon)
Liraglutide (Victoza)
Dulaglutide (Trulicity)
Semaglutide (Ozempic)
Albiglutide (Tanzeum)
Flozins: Oral medications. Increases sugar output in the urine, up to 450 calories per day in glucose. Associated with genital infections.
Generally considered lower risk on its own, can become HIGH RISK when combined with other medications, especially insulin and
sulfonylureas
Canagliflozin (Invokana)
Dapagliflozin (Farxiga)
Empagliflozin (Jardiance)
Ertugliflozin (Stelgatro)
Gliptins: Oral medications. Increase insulin output from pancreas, decrease glucose output from liver. Generally considered lower risk on
their own, can become HIGH RISK when combined with other medications, especially insulin and sulfonylureas
Alogliptin (Nesina)
Linagliptin (Tradjenta)
Sitagliptin (Januvia)
Saxagliptin (Onglyza)
Vildagliptin (Galvus)
Sulfonylureas: Oral medications. Long half-lives ranging from 12-60 hours. These patients are at especially HIGH RISK for recurrent
hypoglycemia and frequently require admission
Clorpropamide (Diabinese)
Glimeperide (Amaryl)
Glipizide (Glucotrol, Glucotrol XL)
Glyburide (Diabeta, Glynase)
Tolazamide (Tolinase)
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2300
HYPERTHERMIA
2300 - HYPERTHERMIA
Care Goals:
Cooling and rehydration
Assess severity of heat-related illness
Mitigate risk for decompensation
Mitigate risk for agitation and uncooperative behavior
Assessment:
Assess ABCs and vital signs
Assess severity of heat-related illness
Heat Cramps:
Muscle cramps usually in legs and abdominal wall. Temperature is normal
Typically sweaty skin signs
Heat Exhaustion:
Prolonged process of salt and water depletion usually of a gradual onset.
As it progresses tachycardia, hypotension, elevated temperature, and very painful cramps occur.
Symptoms of headache, nausea, and vomiting occur.
Vomiting creates a feedback loop that worsens the patient’s salt and water depletion, which can rapidly lead to heat
stroke
Heat Stroke:
Occurs when the cooling mechanism of the body ceases due to temperature overload and/or electrolyte imbalances.
Patient core temperature is usually greater than 104°F.
When no thermometer is available, it is distinguished from heat exhaustion by altered level of consciousness, seizures, or
coma
May be characterized by dry skin signs, however this is not always true, especially in humid conditions
Perform heat illness-related survey:
Ambient temperature and humidity
Oral intake
Exertion level
Length of exposure
Clothing
Availability of water/cooling areas
Signs of alcohol or recreational substance use
Nature of environment (hot warehouse, confined space work, direct sunlight, etc.)
Assess for medical causes of AMS with hyperthermia:
Fever from infectious or inflammatory conditions
History of thyroid disease (especially Grave’s Disease, assess for goiters and/or bulging, staring eyes with limited blinking)
Malignant hyperthermia
Serotonin syndrome
Neuroleptic malignant syndrome
Stimulant drug abuse
Delirium with agitated behavior, especially with prolonged exertion such as running or fighting
Management:
Be mindful of factors that lead to heat emergency – DON’T BECOME A PATIENT
Move patient to a cool area, shield from sun and other heat sources
Pavement temperature can be over 50 degrees higher than air temperatures and conducts heat better than air, causing rapid core
heating and skin burns to both patients and providers
Remove as much clothing as is practical and loosen any restrictive garments.
If alert and oriented AND no suspected medical cause of hyperthermia, give small sips of cool liquids
If altered, check blood glucose
If core temperature is greater than 104o F or if AMS is present:
Expose the patient
Set patient care compartment to maximum AC and fan speed
Place ice packs in the groin, axilla, and behind the neck
Truncal ice packs may be used, but can interfere with and are less effective than evaporation
Continually mist exposed skin with water while fanning victim
If misting is not available, periodically apply and then remove water-soaked towels from exposed skin
DO NOT leave water-soaked linens. This inhibits evaporation and delays cooling.
Begin lights and sirens transport
Additional Considerations:
Patients at elevated risk for heat emergencies include neonates, infants, and patients with mental illness or cognitive
impairment
Contributory risk factors may come from:
Prescription and over-the-counter herbal supplements
Cold medications
Heart medications
Diuretics
Psychiatric medications
Drug abuse
Accidental or intentional drug overdose
Heat exposure can occur either due to increased environmental temperatures or prolonged exercise or a combination of both
Environments with temperature greater than 90°F and humidity greater than 60% present the most risk
Heat stroke is associated with cardiac arrhythmias independent of drug ingestion/overdose
Heat stroke has also been associated with cerebral edema
For patients with signs and symptoms of heat stroke, rapid cooling takes priority over other interventions (e.g., cardiac monitoring,
IV access)
Shivering may occur while treating heat stroke. It is uncertain how harmful shivering is to heat stroke patients.
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2325
HYPOTHERMIA
2325 - HYPOTHERMIA
Care Goals:
Maintain hemodynamic stability
Determine severity of hypothermia
Appropriate management of hypothermia induced cardiac arrest
Prevent further heat loss
Rewarm the patient in a safe manner
Prevent tissue loss
Assessment:
Assess ABCs and vital signs
Patients suffering from moderate or severe hypothermia may have severe alterations to their vital signs including weak and
extremely slow pulses, profound hypotension, and decreased respirations
The rescuer may need to evaluate the hypothermic patient for a pulse for longer than the normothermic patient (up to 60 seconds)
Assess severity of hypothermia. It is not necessary to confirm the temperature, the symptoms describe the severity.
Mild: 32.1°–35°C/89.8°–95°F, vital signs not depressed; normal mental status; shivering is preserved; body maintains the ability
to attempt to control temperature
Moderate: 28.1°–32°C/82.5°–89.7°F, progressive bradycardia, hypotension, and decreased respirations, alterations in mental status
with eventual coma, shivering will be lost in moderate hypothermia (generally between 30°–31°C (86°-87.8°F), and general slowing
of bodily functions
Severe: 24°–28°C/75.2°–82.4°F, progression of above symptoms, body loses ability to regulate temperature.
Assess for frostbite
Patients with frostbite will develop numbness involving the affected body part along with a "clumsy" feeling along with areas of
blanched skin.
Later findings include a "woody" sensation, decreased or loss of sensation, bruising or blister formation, or a white and waxy
appearance to affected tissue
History: along with standard SAMPLE history, additional patient history should include:
Associated injury or illness
Duration of cold exposure
Ambient temperature
Treatments initiated before EMS arrival
Management (Moderate, Severe, Profound):
Maintain patient and rescuer safety
Prevent further heat loss:
Remove the patient from the environment
Remove wet clothes. Clothing should always be cut off. Move the patient’s limbs and body as little as possible.
Dry skin
Insulate from the ground, shelter the patient from wind and wet conditions, and insulate the patient with dry clothing or a
hypothermia wrap/blanket.
If patient is unconscious, apply defibrillator pads
Cover the patient with a vapor barrier (space blanket)
Maintain patient in horizontal position, minimize movement
CAUTION: Motion of the extremities can cause return of significantly colder blood to the heart. Move the patient only when
necessary, such as initial heat loss prevention
Assess responsiveness, breathing, and pulse
Do a pulse check for 60 seconds (clinical signs of death such as dilated pupils are not reliable in the hypothermic patient)
Pulse and breathing absent:
Generally, CPR should not be initiated if the patient:
Is known to have been submerged (head under water) in cold water for more than 90 minutes.
Has obvious signs of death (e.g. decapitation, slippage of skin, animal predation).
Frozen core or airway (e.g. ice formation in the airway).
Has a chest wall that is so stiff that compressions are impossible.
For "Shock Indicated”, defibrillate ONCE
Withhold further shocks and transport immediately.
Obtain IV/IO access.
Warm packs should not be used.
For “No Shock Indicated”,
Obtain IV/IO access
Warm packs should not be used
For patients with a pulse and spontaneous respirations:
Begin oxygen therapy.
Begin transport immediately.
Rewarming according to severity:
Mild hypothermia (temperature greater than or equal to 92o F or if the patient
is shivering) - Passive rewarming, active external rewarming.
Moderate hypothermia (temperature greater than or equal to 86o F to less than
92o F, or if patient is shivering) - Passive rewarming, active external rewarming to truncal areas only (neck, armpits,
groin).
Severe hypothermia (temperature less than 86o F) - Transport for active internal
rewarming.
In patients suffering from moderate to severe hypothermia, it is critical to not allow these patients to stand or exercise as this may
cause circulatory collapse
Frostbite care:
If the patient has evidence of frostbite, and ambulation/travel is necessary for evacuation or safety, avoid rewarming of extremities
until definitive treatment is possible. Additive injury occurs when the area of frostbite is rewarmed then inadvertently refrozen.
Only initiate rewarming if refreezing is absolutely preventable
Rewarm frostbitten parts by contact with nonaffected body surfaces. Do not rub or cause physical trauma.
After rewarming, cover injured parts with loose sterile dressing. Do not allow injury to refreeze.
Transport to a BURN CENTER
Considerations:
Shivering rapidly converts calories to body heat. If patient’s mental status is declining, check blood glucose and treat as indicated
(treat per Hypoglycemia Guideline or Hyperglycemia Guideline) and assess for other causes of alterations of mentation.
Monitor frequently — if temperature or level of consciousness decreases, refer to severe hypothermia
Rectal temperatures are the most accurate prehospital temperature, but take with caution to avoid worsening the hypothermia by
undressing the patient. The insertion may cause the patient to vagal, worsening bradycardia
If supporting respirations, care must be taken not to hyperventilate the patient as hypocarbia may reduce the threshold for ventricular
fibrillation in the cold patient. If possible, use EtCO2 with a target of 35-45.
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2350
HYPOVOLEMIA/SHOCK
2350 - HYPOVOLEMIA/SHOCK
Care Goals:
Rapidly recognize shock and perform BLS interventions maintain/restore adequate perfusion to vital organs
Differentiate between possible underlying causes of shock to promptly initiate additional therapy
Assessment:
Assess ABCs and vital signs
If concerned for shock, assess for signs of poor perfusion (due to a medical cause) such as one or more of the following:
Altered mental status
Delayed capillary refill (> 3 seconds)
Flash capillary refill (> 1 second) may be seen in early septic shock
Decreased urine output
Respiratory rate greater than 20 per minute in adults
Assess potential etiologies of shock:
Hypovolemic (hemorrhagic or non-hemorrhagic, such as severe dehydration, vomiting or diarrhea)
Patients with adrenal insufficiency may have an emergency dose of hydrocortisone available that can be administered IV or IM
History of a solid organ or bone marrow transplant
Infants
Elderly
In most adults, tachycardia is the first sign of compensated shock, and may persist for hours. Tachycardia can be a late sign of
shock in children and a tachycardic child may be close to cardiovascular collapse
Hypotension indicates uncompensated shock, which may progress to cardiopulmonary failure within minutes. Hypotension is a late
and ominous sign in pediatric uncompensated shock
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2400
OB PREGNANCY/LABOR/DELIVERY
2400 - OB PREGNANCY/LABOR/DELIVERY
Care Goals:
Obtain necessary history to plan for birth and resuscitation of the newborn
Recognize imminent birth
Plan for resources based on number of anticipated patients (e.g., mother and child or multiple births)
Assist with uncomplicated delivery of term newborn
Recognize complicated delivery situations (e.g., nuchal or prolapsed umbilical cord, breech delivery, shoulder
dystocia) and plan for management and appropriate transport destination
Apply appropriate techniques when an obstetric complication exists
Assessment:
Assess for signs of imminent delivery:
Crowning or other presentation in vaginal opening
Urge to push
Urge to move bowels
Mother’s sense of imminent delivery
Assess for signs of active labor:
Contractions
Membrane rupture
Bloody show
Management:
If patient is imminently delivering, prepare to provide delivery care
Delivery should be controlled to allow a slow controlled delivery of infant – This will prevent injury to mother
Support the infant’s head as needed and apply gentle counterpressure to help prevent the head from suddenly popping out
Check for nuchal cord (i.e., around the baby’s neck)
If present, slip it over the head
If unable to free the cord from the neck, double clamp the cord and cut between the clamps
Do not routinely suction the infant’s airway (even with a bulb syringe) during delivery
Grasping the head with hand over the ears, gently guide head down to allow delivery of the anterior shoulder
Gently guide the head up to allow delivery of the posterior shoulder
Slowly deliver the remainder of the infant
After 1 minute, clamp cord about 5–6 inches from the abdomen with two clamps; cut the cord between the clamps
If resuscitation is needed, the baby can still benefit from a 1-minute delay in cord clamping. Start resuscitation immediately
after birth and then clamp and cut the cord at 1 minute
While cord is attached, take care to ensure the baby is not significantly higher positioned than the mother to prevent blood
from flowing backwards from baby to placenta
Dry, warm, and stimulate infant wrap in towel and place on maternal chest unless resuscitation needed
Resuscitation takes priority over recording APGAR scores. Record APGAR scores at 1 and 5 minutes once neonate is stabilized
After delivery of infant, suctioning (including suctioning with a bulb syringe) should be reserved for infants who have obvious
obstruction to the airway or require positive pressure ventilation (follow Neonatal Resuscitation Guideline for further care of
the infant)
The placenta will deliver spontaneously, often within 5–15 minutes after the infant is delivered
Do not force the placenta to deliver; do not pull on the umbilical cord
Contain all tissue in plastic bag and transport
After delivery, massaging the uterus (should be located at about the umbilicus) and allowing the infant to nurse will promote uterine
contraction and help control bleeding
Keep infant warm during transport
Most deliveries proceed without complications – if complications can’t be resolved in the field
Apply high flow oxygen to mother and expedite transport to the appropriate receiving facility
Considerations: The following are recommendations for specific complications:
Shoulder dystocia – if delivery fails to progress after head delivers, quickly attempt the following:
Hyperflex mother’s hips to severe supine knee-chest position (i.e., McRoberts’ maneuver)
Attempt to angle baby’s head as posteriorly as possible but NEVER pull
Continue with delivery as normal once the anterior shoulder is delivered
Prolapsed umbilical cord
Placed gloved hand into vagina and gently lift head/body off the cord
Assess for pulsations in cord, if no pulses are felt, lift the presenting part off the cord
Wrap the prolapsed cord in moist sterile gauze
Maintain until relieved by hospital staff
If previous techniques are not successful, mother should be placed in prone kneechest position or extreme Trendelenburg with hips
elevated
Breech birth
Place mother supine, allow the buttocks, feet, and trunk to deliver spontaneously, then support the body while the head is
delivered
If needed, put the mother in a kneeling position which may assist in the delivery of the newborn
Assess for presence of prolapsed cord and treat as above
If head fails to deliver, place gloved hand into vagina with fingers between infant’s face and uterine wall to create an open airway.
Place your index and ring fingers on the baby’s cheeks forming a “V” taking care not to block the mouth and allowing the chin to be
tilted toward the chest flexing the neck
When delivering breech, you may need to rotate the baby’s trunk clockwise; or sweep the legs from the vagina
Once the legs are delivered support the body to avoid hyperextension of the head; keep the fetus elevated off the umbilical cord
NEVER pull on the body, especially a preterm or previable baby – just support the baby’s body while mother pushes when she feels the
urge to
The presentation of an arm or leg through the vagina is an indication for immediate transport to hospital
Nuchal Cord
After the head has been delivered, palpate the neck for a nuchal cord, if present, slip over the head
If the loop is too tight to slip over the head, attempt to slip the cord over the shoulders and deliver the body through the loop
The cord can be doubly clamped and cut between the clamps; the newborn should be delivered promptly
Maternal Cardiac Arrest
Apply manual pressure to displace uterus from midline
Treat per the Cardiac Arrest Guideline (VF/VT/Asystole/PEA) for resuscitation care (defibrillation and medications should be given
for same indications and doses as if non-pregnant patient)
Transport as soon as possible if infant is estimated to be over 24 weeks gestation (perimortem Cesarean section (also known as
resuscitative hysterotomy) at receiving facility is most successful if started within 5 minutes of maternal cardiac arrest)
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2425
POISONING/DRUG INGESTION
2425 - POISONING/DRUG INGESTION
Care Goals:
Rapid recognition and intervention of a clinically significant opioid poisoning or overdose
Differentiation of opioid intoxication from other medical emergencies, such as head injuries, strokes, hypoglycemia, or other
toxidromes
All altered patients requiring respiratory support should be ventilated with high flow O2 via bag-valve-mask device.
For any patient with a respiratory rate less than eight, or a patient history of or physical findings consistent with opioid
overdose
Maintaining the patients airway and respiratory status takes priority over medications Consider naloxone hydrochloride (Narcan)
-0.4 mg up to 2 mg IM/IN.
NOTE: For all IN doses that are ≤ 0.9 mL, add 0.1 mL to ensure full dose of medication is given.
Due to the relatively short half-life of naloxone hydrochloride (Narcan), patients that respondglutose favorably to naloxone (Narcan)
administration should still be considered under the influence and transported on a peace/health officer hold (aka transport hold)
regardless of their mental status and/or refusal of care.
If the patient has a history of COPD and is symptomatic (presence of wheezing alone does not indicate COPD), en route to hospital,
the following may be administered:
Use a nasal cannula at 2 – 3 liters per minute initially. Oxygen may need to be increased if the patient’s oxygenation status
worsens.
When a patient is already on oxygen, EMS oxygen therapy flow rate should not start at a lower rate than the patient’s current
rate.
Oxygen flow should be titrated to a target SpO2 of 90%.
Supplemental oxygen for non-COPD related dyspnea to a target 94-98% SpO2
For suspected bronchospasm, asthma, COPD
Nebulized medications (may nebulize continuously without improvement):
Consider CPAP if two or more of the following are present:
Retractions or accessory muscle use.
Pulmonary edema.
Respiratory rate greater than 25/min.
SpO2 less than 92%.
Administer BiLevel CPAP to achieve 11 - 12 cm H2O IPAP (16 LPM) with EPAP set to lowest possible pressure. If
oxygenation status doesn't improve, increase EPAP to achieve desired SpO2.
Assess the patient’s response. If the patient’s condition worsens, (e.g. the patient becomes hypotensive, decreased SpO2)
discontinue CPAP.
If CPAP is initiated, continue to treat with medications as normal.
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2500
SEIZURES
2500 - SEIZURES
Care Goals:
Prompt cessation of seizures in the prehospital setting
Minimizing adverse events in the treatment of seizures in the prehospital setting
Identifying treatable causes of seizure
Minimizing seizure recurrence during transport
Assessment:
History:
Duration of current seizure
Prior history of seizures, diabetes, alcohol or medication abuse.
Typical appearance of seizures
Baseline seizure frequency and duration
Focality of onset, direction of eye deviation
Concurrent symptoms of apnea, cyanoisis, vomiting, bowwel/bladder incontience, or fever
Bystander administration of medications to stop the seizure
Current medications, includijng anticonvulstants
Recent dose cahnges or non-complinace with anticonvulstants
History of trauma, pregnancy, heat exposure, or toxin exposure
Exam:
Airway Patency
Respiratory rate and effectiveness of patient’s breathing
Signs of perfusion
Neurologic status
GCS
Nystagmus
Pupil size
Focal deficits such as paralyzed limbs or other evidence of stroke
Management:
If signs of airway obstruction are present and chin-lift, jaw thrust, position, and/or suctioning do not accomplish a patent airway,
place an OPA or NPA (if gag present)
Monitor SpO2
Administer oxygen as appropriate with a target of achieving 94-98%
If seizure activity is suspected from eclampisa (>20 weeks gestation with hypertension or up to 7 days postpartum
Begin immediate transport and notify receiving facility of suspected eclamptic seizure
Considerations:
For reported first time seizures or seizures that are refractory to medication, consider other potential causes:
Head Trauma
Hypoglycemia
Stroke
Electrolyte problems
Toxins
Pregnancy with eclampsia
Hyperthermia
Consider syncope versus seizure in a first-time seizure patient. Due to the frightening appearance of some syncopal episodes, bystanders
may describe seizure-like activity that occurs during syncope.
The presence of fever with seizure in children less than 6 months old and greater than 6 years old is not consistent with a simple
febrile seziure and should prompt concern for meningitis, encephalitis, or other pathology
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2625
CHEMICAL BURNS
2625 - CHEMICAL BURNS
Care Goals:
Rapid recognition of topical chemical burns
Initiation of emergent and appropriate intervention and transport
Assessment:
Before attempting any assessment or care, don the appropriate PPE
Remove patient’s clothing if necessary
Contaminated clothing should preferably be placed in double bags
Information about the chemical should be gathered while on scene including materials safety data sheet if available
Communicate all data regarding the chemical to the receiving facility
Clinical effects and severity of a topical chemical burn is dependent upon:
Class of agent (alkali injury or acid injury)
Concentration of the chemical (the higher the concentration, the greater the risk of injury)
pH of the chemical
Alkali-increased risk with pH greater than or equal to 11
Acid-increased risk with pH less than or equal to 3
Pay special attention to assessment of ocular or oropharyngeal exposure
Evaluate for hoarseness, complaints of sore throat, coughing, or other symptoms associated with inhalation or ccontact injuries
Monitor for laryngospasm (stridor) and bronchospasm (wheezing)
Management:
Do not attempt to neutralize acids or bases. These reactions release energy in the form of heat, potentially causing thermal
burns.
If dry chemical contamination, carefully brush off solid chemical prior to flushing the site as the irrigating solution may activate
a chemical reaction
If wet chemical contamination, flush the patient’s skin (and eyes, if involved) with copious amounts of water or normal saline
Take measures to minimize hypothermia
If the suspected chemical is Hydroflouric Acid (HF),
HF is a highly corrosive substance used for automotive cleaning products, rust removal, porcelain cleaners, etching glass, cleaning
cement or brick.
HF readily penetrates intact skin and causes underlying tissue injury with few or no outward signs. Higher concentrations cause more
obvious signs, but low concentrations can still cause severe injury
For all patients in whom a hydrofluoric acid exposure is confirmed or suspected:
Vigorously irrigate all affected areas with water or normal saline for a minimum of 15 minutes
Apply AED pads for oral or large dermal exposures significant HF exposures
Since the severity of topical chemical burns is largely dependent upon the type, concentration, and pH of the chemical involved as well
as the body site and surface area involved, it is imperative to obtain as much information as possible while on scene about the chemical
ubstance by which the patient was exposed. The information gathering process will often include:
Transport of the original or a copy of the Material Safety Data Sheet (MSDS) of the substance to the receiving facility
Contacting the reference agency to identify the chemical agent and assist in management (e.g., CHEMTREC®)
Inhalation of HF should be considered in any dermal exposure involving the face and neck or if clothing is soaked in the product
Decontamination is critical for both acid and alkali agents to reduce injury — removal of chemicals with a low pH (acids) is more
easily accomplished than chemicals with a high pH (alkalis) because alkalis tend to penetrate and bind to deeper tissues
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2640
THERMAL BURNS
2640 - THERMAL BURNS
Care Goals:
Ensure crew safety
Minimize tissue damage and morbidity from thermal burns
Prevent infection
Minimize pain
Assessment:
Circumstances of event – Consider:
Trauma in addition to burns
Inhalation exposures such as carbon monoxide (CO) and cyanide (CN)
Mouth and nares – patients with redness, blisters, soot, singed hairs have presumptive airway involvement
Breathing – rapid, shallow, wheezes, rales
Skin – Estimate Total Burn Surface Area (TBSA) and depth (partial vs. full thickness)
Superficial burns are not included in TBSA
Associated trauma – blast, fall, assault
Management:
Wait until trained responders have verified:
PPE Requirements
Electrical lines secure
Gas off
No secondary devices
Hazmat determinations made
Stop the burning
Remove wet clothing (if not stuck to the patient)
Remove jewelry
Leave blisters intact
If burns are tar-related, do not apply water to hot tar. Apply dish soap to outside of tar, then wrap in moist dressing
Minimize burn wound contamination
Cover burns with dry dressing or clean sheet
Do not apply gels or ointments
Monitor Vitals
Regardless of the SPO2 and EtCO2, high flow supplemental oxygen for all burn patients rescued from an enclosed space,
including any indoor fire
CAUTION: Shock and hypotension from burns can take up to an hour to occur. If the patient has a fresh burn and is in shock or
unconcious, be highly concerned for a different cause, such as toxins (cyanide, CO), dysrhythmia, trauma, or hypoxia.
Consider direct transport to a burn center for major burns (2100 - Patient Disposition - Major Burns). Hospitals
in the Twin Cities Metro area with a burn unit include:
Hennepin County Medical Center
Regions Medical Center
Major burn criteria includes:
Partial-thickness burns greater than 10% of total body surface area.
Partial-thickness or third degree burns that involve the face, hands, feet, genitalia, perineum, or major joint.
Third degree burns in any age group.
Lightning injury and other electrical burns.
Chemical burns.
Inhalation injury.
Burn in any patients with preexisting medical disorders that could complicate management, prolong recovery, or affect
mortality.
For any significant burn:
Begin oxygen therapy. Use positive pressure ventilatory assist as needed.
Patients with burns that encircle the torso are at risk for ventilatory compromise, monitor closely for declining
breathing.
Apply sterile dressings and saturate with cool water (leave Gel-pack(s) in place if applied by first responders).
Do not allow any burn patient to become chilled and begin shivering.
If more than 20% of the body surface is burned:
Burns that involve significant sloughing or loss of skin can result in uncontrolled heat loss. These patients should be
monitored closely for the development of hypothermia and appropriate preventative measures should be taken
Remove any non-adherent burned clothing and cover the patient with a sterile sheet.
Do not cool down with water.
Begin rapid transport.
Consider direct transport to a burn center for major burns.
Apply AED pads after any electrical burn including a lightning strike.
Considerations:
Have a high index of suspicion for cyanide poisoning in a patient with depressed GCS, respiratory difficulty, and cardiovascular collapse
in the setting of an enclosed-space fire.
These patients likely require hyperbaric therapy and should be transported to HCMC or Regions
Particularly in enclosed-space fires, carbon monoxide toxicity is a consideration and pulse oximetry may not be accurate
[See 3430 - Carbon Monoxide (CO) Poisoning]
Onset of stridor and change in voice are sentinel signs of potentially significant airway burns, which may rapidly lead to airway
obstruction or respiratory failure.
2640 - Burns Sale
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2675
ELECTROCUTION
2675 - ELECTROCUTION
Care Goals:
Prevent additional harm to patient
Identify life threatening issues such as dysrhythmias and cardiac arrest
Identify characteristics of electrical source to communicate to receiving facility (voltage, amperage, alternating
current [AC] versus direct current [DC])
Assessment:
Verify scene is secure.
The electrical source must be disabled prior to assessment
Perform primary survey with specific focus on dysrhythmias or cardiac arrest—apply AED as soon as feasible
Identify all sites of burn injury. If the patient became part of the circuit, there will be an additional site near the contact
with ground. Electrical burns are often full thickness and involve significant deep tissue damage, and there may be multiple burn
sites
Assess for potential associated trauma and note if the patient was thrown from contact point. If patient has altered mental status,
assume trauma was involved and treat accordingly
Determine characteristics of source if possible (AC or DC, voltage, amperage, time of injury)
Management:
Identify dysrhythmias or cardiac arrest — even patients who appear dead (particularly dilated pupils) may have good outcomes with prompt
intervention [see appropriate guideline for additional information and patient assessment/treatment]
Remove constricting clothing and jewelry since additional swelling is possible
Consider direct transport to a burn center for major burns. Hospitals in the Twin Cities Metro area with a burn unit include:
Hennepin County Medical Center
Regions Medical Center
Considerations:
Electrical current causes injury through three main mechanisms:
Direct tissue damage, altering cell membrane resting potential, and eliciting tetany in skeletal and/or cardiac muscles
Conversion of electrical energy into thermal energy, causing massive tissue destruction and coagulative necrosis
Mechanical injury with direct trauma resulting from falls or violent muscle contraction
Anticipate cardiac arrest
The mortality related to electrical injuries is impacted by several factors:
Path through the body- electricity crossing the heart has higher mortality
Type of current (AC vs. DC)
AC is more likely to cause cardiac dysrhythmias while DC is more likely to cause deep tissue burns however either type of
current can cause any injury
DC typically causes one muscle contraction while AC can cause repeated contractions
Both types of current can cause involuntary muscle contractions that do not allow the victim to let go of the electrical
source
AC is more likely to cause ventricular fibrillation while DC is more likely to cause asystole
The amount of current impacts mortality more than the voltage
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
BLS Protocols
2700
SPINAL INJURIES
2700 - SPINAL INJURIES
Care Goals:
Select patients for whom spinal motion restriction (SMR) is indicated
Minimize secondary injury to spine in patients who have, or may have, an unstable spinal injury
Minimize patient morbidity from the unnecessary use of immobilization devices
Assessment:
Assess the scene to determine the mechanism of injury
Mechanism alone should not determine if a patient requires spinal motion restriction – however, mechanisms that have been
associated with a higher risk of injury are:
Motor vehicle crashes (including automobiles, all-terrain vehicles, and snowmobiles)
Axial loading injuries to the spine
Falls greater than 10 feet
Assess the patient in the position found for findings associated with spine injury:
Mental status
Neurologic deficits
Spinal pain or tenderness
Any evidence of intoxication
Other severe injuries, particularly associated torso injuries
Management:
Place patient in cervical collar and initiate spinal motion restriction in adults if there are any of the following:
Patient complains of midline neck or spine pain
Any midline neck or spinal tenderness with palpation
Any abnormal mental status (including extreme agitation)
Focal or neurologic deficit
Any evidence of alcohol or drug intoxication
Another severe or painful distracting injury
A communication barrier that prevents accurate assessment
If none of the above apply, patient may be managed without a cervical collar
Patients with penetrating injury to the neck should not be placed in a cervical collar or other spinal precautions regardless
of whether they are exhibiting neurologic symptoms or not. Doing so can lead to delayed identification of injury or airway compromise
and has been associated with increased mortality
If extrication is required:
From a vehicle: After placing a cervical collar, if indicated, children in a booster seat and adults should be allowed to
self-extricate. For infants and toddlers already strapped in a car seat with a built-in harness, extricate the child while
strapped in his/her car seat
Other situations requiring extrication: A, preferably padded, long board may be used for extrication, using the lift and slide
(rather than a logroll) technique
Helmet removal
If a football helmet needs to be removed, it is recommended to remove the face mask followed by manual removal (rather than the
use of automated devices) of the helmet while keeping the neck manually immobilized — occipital and shoulder padding should be
applied, as needed, with the patient in a supine position to maintain neutral cervical spine positioning
Evidence is lacking to provide guidance about other types of helmet removal
Do not transport patients on rigid long boards unless the clinical situation warrants long board use. An example of this may be
facilitation of immobilization of multiple extremity injuries or an unstable patient where removal of a board will delay transport
and/or other treatment priorities.
Patients should be transported to the nearest appropriate facility, in accordance with the American College of Surgeons Committee on
Trauma (ACS COT) 2022 National Guideline for the Field Triage of Injured Patients
Patients with severe kyphosis or ankylosing spondylitis may not tolerate a cervical collar. These patients should be immobilized in
a position of comfort using towel rolls. Ideally, take an additional first responder to assist.
Considerations:
Safety concerns associated with immobilization:
Be aware of potential airway compromise or aspiration in immobilized patient with nausea/vomiting or with facial/oral bleeding
Excessively tight immobilization straps can limit chest excursion and cause hypoventilation
Prolonged immobilization on spine board can lead to ischemic pressure injuries to skin
Prolonged immobilization on spine board can be very uncomfortable for patient
Children are abdominal breathers therefore immobilization straps should go across chest and pelvis and not across the abdomen
Children have disproportionately larger heads. When securing pediatric patients to a spine board, the board should have a recess for
the head or the body should be elevated approximately 1–2 cm to accommodate the larger head size and avoid neck flexion when
immobilized
In an uncooperative patient, avoid interventions that may promote increased spinal movement
The preferred position for all patients with spine management is flat and supine. There are three circumstances under which raising
the head of the bed to 30 degrees may be considered:
Respiratory distress
Suspected severe head trauma
Promotion of patient compliance
Pediatric considerations:
Age alone should not be a factor in decision-making for prehospital spine care, yet the patient’s ability to reliably be assessed at
the extremes of age should be considered. Communication barriers with infants/toddlers or elderly patients with dementia may prevent
the clinician from accurately assessing the patient
Because of variation in head size to body ratio, consider additional padding under the shoulders to avoid excessive cervical spine
flexion
Ambulatory patients may be safely immobilized on gurney with cervical collar and straps and will not generally require a spine
board.
The role for standing take downs is extremely limited, e.g., extrication of a patient with a high likelihood of a spinal cord injury
from a large body of water.
Ambulatory patients may have a collar applied and walked to the EMS gurney
Reserve long spine board use for the movement of patients whose injuries limit ambulation and who meet criteria for the use of spinal
precautions. Remove from the long board as soon as is practical.
Impedes clotting by blocking prostaglandin synthesis, which prevents formation of the platelet-aggregating substance
thromboxane A2
Indications:
Provider Impression Chest Pain/ Discomfort of suspected Cardiac origin.
Contraindications:(do NOT give if)
Hypersensitivity (allergy) to drug.
Patients with active ulcer disease.
Dose:
Give 324 mg of chewable ASA give within minutes of arrival.
Side Effects:
Use with caution in patients with GI lesions, impaired renal function, hypoprothrombinemia (anticoagulation therapy),
vitamin K deficiency, thrombocytopenia, or severe hepatic impairment.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Medication Administration
Guideline Number - 3050
BENADRYL
3050 - BENADRYL
Medication Name:
Benedryl
Actions:
Antihistamine
Indications:
Provider Impression of Anaphylaxis / Allergic Reaction.
Contraindications: (do NOT give if)
Hypersensitivity to diphenhydramine.
Newborns or premature infants.
Nursing mothers.
Precautions:
May cause drowsiness, especially in the elderly.
Use with caution in patients with glaucoma.
May potentiate the effects of other sedative and psychiatric agents, especially the MAO inhibitors, with which it should not
be used.
Dose:
Adult Dose: 25-50 mg ORALLY
Note: Liquid preparation is preferred over tablets.
Side Effects:
Common
Dizziness
Dryness of mouth, nose, or throat.
Sedation, sleepiness.
Thickening of bronchial secretions
Serious
Anaphylaxis
Administration:
In adult patients presenting signs and symptoms of anaphylaxis and under the direction of medical
control, administer 25 mg of Benadryl ORALLY.
In pediatric patients presenting signs and symptoms of anaphylaxis and under the direction of
medical control, administer 1mg/kg (1 kg = 2.2 lbs) of Benadryl ORALLY.
If service is unable to contact medical control and signs and symptoms of anaphylaxis are severe,
give 25 mg ORALLY (adult) or
1mg/kg (1 kg = 2.2 lbs) ORALLY (pediatric age 1-12,if under age 1 contact medical control for direction). Continue to attempt contact
with medical direction.
(OPTIONAL) Requires EMSRB Variance Approval per Minnesota Rules 4690.8300 SPECIFIC VARIANCES Subpart7
Medication Name:
Albuterol
Actions:
Dilates bronchioles
Indications:
Provider Impression:
Asthma
Respiratory Distress - COPD
Allergic Reaction
CHF/Pulmonary Edema
Contraindications:
Patient is unable to use the device (not alert or unable to be coached).
Dose:
1 or 2 inhalations every 10 minutes. Contact medical control if not improved after
2nd dose.
Metered Dose Inhaler Administration:
Check right medication, expiration date.
Use a spacer.
Assure the inhaler is at room temperature.
Shake canister vigorously.
Ask patient to exhale deeply and place lips around inhaler opening.
Ask patient to inhale slowly and deeply as they depress the canister.
Have the patient hold their breath for as long as comfortably possible.
Resume oxygen administration.
Repeat second inhalation as needed in approximately one minute.
Side Effects:
increases pulse rate, causes tremors or nervousness
Ongoing Assessment:
Continue to assess and monitor airway, breathing, circulation and level of consciousness.
Continue high-flow oxygen.
Take frequent vital signs (pulse, respirations, and blood pressure).
Observe for deterioration and assist patient with additional puffs of inhaler and/or be prepared to assist ventilations.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Medication Administration
Guideline Number - 3140
BETA-AGONIST MEDICATION NEBULIZER
3140 - BETA-AGONIST MEDICATION NEBULIZER
(OPTIONAL) Requires EMSRB Variance Approval per Minnesota Rules 4690.8300 SPECIFIC VARIANCES Subpart7
Medication Name:
Albuterol, Proventil, Ventolin
Actions:
Dilates bronchioles
Indications:
Provider Impression:
Asthma
Respiratory Distress - COPD
Allergic Reaction
CHF/Pulmonary Edema with wheezing
Contraindications:
Patient is unable to use the device (not alert or unable to be coached).
Hypersensitivity to Albuterol.
Dose: Ages 1 and up - 1 unit dose every 10 minutes from the completion of previous dose as needed. CONTACT MEDICAL CONTROL if not improved after second administration.
Using A Nebulizer:
Put the liquid medication in the chamber.
Attach oxygen tubing to the chamber and set the flow rate at 6 – 8 lpm.
Observe the medication mist coming from the device.
Have the patient seal their lips around the mouthpiece and breathe deeply or attach the face mask to the chamber and
administer via the mask.
Instruct the patient to hold their breath for a few seconds after breathing if possible.
Continue until the medication is gone from the chamber.
Reassess the patient’s level of distress and vital signs.
Document the patient’s response to the medication.
Pediatric Considerations:
May be administered via Blow By method if child is too young to hold in mouth.
For ages less than 1 year of age, Contact Medical Control.
Ongoing Assessment:
Continue to assess and monitor airway, breathing, circulation and level of consciousness. Continue high-flow oxygen.
Take frequent vital signs (pulse, respirations, and blood pressure).
Observe for deterioration and assist patient with additional puffs of inhaler and/or be prepared to assist ventilations.
Monitor the patients level on consciousness closely as decreasing level of consciousness is often the first sign of impending
respiratory failure.
Provider Impression Altered Level of Consciousness (Blood Glucose Level not obtainable)
Contraindications: (do NOT give if)
Any patient who cannot control their own airway.
Dose:
Give 25 grams orally.
Precaution:
Airway must be carefully maintained.
Administration:
Perform blood glucose measurement.
Administer 1 tube (Dextrose (D50W)/Glutose = 25gm per tube) by mouth.
DO NOT ADMINISTER IF THE PATIENT CANNOT SWALLOW ON THEIR OWN!
Repeat blood glucose measurement.
Notify medical control that oral glucose has been given.
Pediatric Considerations:
The initial dosage is usually one half of the adult dose.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Medication Administration
Guideline Number - 3200
EPINEPHRINE AUTO INJECTOR
3200 - EPINEPHRINE AUTO INJECTOR
(OPTIONAL) Requires EMSRB Variance Approval per Minnesota Rules 4690.8300 SPECIFIC VARIANCES Subpart 7
Medication Name:
Epinephrine, Adrenaline, EpiPen or EpiPen Jr.
Actions:
Dilates the bronchioles and constricts blood vessels.
Indications:
Provider Impression Anaphylaxis.
Contraindications:
None when used in life threatening situation.
Dose:
Adult (or Child > 60 lbs) - One auto-injector (0.3 mg) repeat in 10 minutes if not
improved.
Infant & Children (< 60 lbs) - One Junior auto-injector (0.15 mg) repeat in 10 minutes if not
improved.
Epi-Pen Administration:
Remove one red cap from epi kit.
For children, Clean injection port on epi vial, and the injection site on the patient
with alcohol or chloraprep; using 0.3 ml syringe, draw 0.3 ml of fluid from the vial: without contaminating the
needle plunge the needle into the injection site, inject the fluid, withdraw the syringe and place into a sharps
container immediately; massage the injection site.
For adults, Clean injection port on epi vial, and the injection site on the patient
with alcohol or chloraprep; using 0.5 ml syringe, draw 0.5 ml of fluid from the vial: follow the remaining directions
as for child above.
Continue to assess and monitor airway, breathing and circulation. Continue high-flow oxygen; take frequent vital signs
(pulse, respirations, blood pressure). Treat for shock as needed and be prepared to provide life support (BVM, CPR, and
AED).
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Medication Administration
Guideline Number - 3225
GLUCAGON, IM
3225 - GLUCAGON, IM
(OPTIONAL) Requires EMSRB Variance Approval per Minnesota Rules 4690.8300 SPECIFIC VARIANCES Subpart 7
Medication Name:
Glucagon, GlucaGen
Actions:
Induces liver glycogen breakdown, releasing glucose into the bloodstream.
Indications:
Provider Impression:
Diabetic Hypoglycemia
Blood Glucose Level of 60 mg/dL with symptoms
Altered Level of Consciousness
Suspected Hypoglycemia in the absence of a blood glucose reading.
Contraindications:
Known hypersensitivity to drug, and in patients with pheochromocytoma or with insulinoma (tumor of pancreas).
Dosage:
1 mg IM for patients over 22 lbs (11 kg).
Glucagon Administration:
Dissolve the powdered glucagon with the accompanying liquid.
Glucagon should not be used at concentrations greater than 1 mg/mL (1 unit / mL).
Glucagon solutions should not be used unless they are clear and of a water-like consistency.
For Adults and children weighting more than 22 lbs give 1 mg (1 unit) by Intra-muscular injection.
Side Effects:
Hyperglycemia (excessive dosage), nausea and vomiting hypersensitivity reactions (anaphylaxis, dyspnea, hypotension, rash),
increased blood pressure, and pulse; this may be greater in patients taking beta-blocker medications.
Precautions:
Give with caution to patients that have low levels of releasable glucose (e.g., adrenal insufficiency, chronic hypoglycemia,
and prolonged fasting).
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Medication Administration
Guideline Number - 3260
NALOXONE (NARCAN)
3260 - NALOXONE (NARCAN)
Medication Name:
Naloxone, Narcan
Actions:
Naloxone displaces the opioid from the opioid receptor in the nervous system and blocks the actions of the opioid.
A single dose’s effects can last as short as 30 minutes.
Indications:
Known opioid overdose; including Codeine, Fentanyl, hydrocodone, hydromorphone, methadone, morphine, oxycodone, lorcet,
Lortab, norco, vicoden, Percocet, Percodan, opium and heroin.
Patients that have been prescribed an opioid and show symptoms of toxicity including; Miosis (pinpoint pupils) Respiratory
depression Decreased mental status.
Contraindications:
Known allergy or hypersensitivity to naloxone.
Precautions:
The administration of naloxone may results in the rapid onset of the signs and symptoms of opioid withdrawal: Agitation,
tachycardia, pulmonary edema, nausea, vomiting and possibly seizures.
Prior to the administration of naloxone all patients should receive the appropriate medical treatment to provide support of
their airway, breathing and circulation (ABC’s).
Prior to the administration of naloxone all patients should be assessed for other causes of altered mental status and/or
respiratory depression such as hypoxia, hypoglycemia, head injury, shock and stroke.
The adverse effects following naloxone administration, especially in chronic opioid users may place the patient, bystanders
and EMS personnel at risk of injury.
Due to the potential adverse effects of naloxone administration, you may consider limiting its use to patients with known or
suspected opioid overdoses with impending cardiopulmonary arrest, severe respiratory depression and shock.
Administration: (Intranasal)
Assemble plastic syringe and glass vial (if applicable)
Attach nasal atomizing device (if applicable)
Insert in nostril at about 45 degree angle
If nasal airway in place, temporarily remove for medication administration.
Briskly inject 1ml (1mg) of naloxone in each nostril – Total Dose: 2 mg IN (or per delivery device specifications, total
dose 2-4mg).
Continue ventilatory assistance, supplemental oxygen and suction as needed.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Medication Administration
Guideline Number - 3275
NITROGLYCERIN
3275 - NITROGLYCERIN
(OPTIONAL) Requires EMSRB Variance Approval per Minnesota Rules 4690.8300 SPECIFIC VARIANCES Subpart 7
Medication Name:
Nitroglycerin, Nitrostat, Nitrolingual, Nitrodur
Actions:
Relaxes or dilates blood vessels and decrease the workload of the heart.
Indications:
Provider Impression:
Chest Pain/Discomfort of Suspected Cardiac Origin
CHF/ Pulmonary Edema
Contraindications:
Patient’s systolic blood pressure is less than 100.
The patient has taken medications for Erectile Dysfunction within the past 48 hours.
Hypersensitivity to Nitroglycerin.
Dosage: (Ages 18 and over)
One tablet sublingual or spray lingual every 5 minutes until symptoms relieved.
Stop if systolic blood pressure drops below 100mm/Hg.
NOTE: Contact Medical Control if not improved after 3 doses.
Nitroglycerin Administration:
Make sure Nitroglycerin is indicated and the patient has no contraindications.
Take blood pressure.
Ask patient to lift tongue and place one tablet or spray dose under tongue (while wearing gloves) or have patient
place tablet or spray under tongue.
Have patient keep mouth closed with tablet under tongue (ask them not to swallow) until the tablet or spray is
dissolved.
Repeat a blood pressure and reassess the patient’s symptoms.
Continue to assess and monitor airway, breathing, and circulation. Maintain adequate SpO2; take frequent
vital signs (pulse, respirations, and blood pressure).
rev. 1 June 2024
rev. 1 June 2024
Ridgeview Ambulance Protocols
Medication Administration
Guideline Number - 3300
OXYGEN
3300 - OXYGEN
Action:
Increases arterial oxygen tension (SaO2) and hemoglobin saturation.
Indications:
Low Flow (1-6 L/min per nasal cannula):
Patients with SpO2s < 96% and respiratory symptoms.
COPD with SpO2 < 90%
Suspected MI (heart attack) with SpO2 < 92%
Suspected CVA with SpO2 < 94%
High Concentration (60 - 100%)
Smoke, carbon monoxide, or toxic gas inhalation.
Hypoxia, (pulse oximetry readings of 96%) from any cause not responding to low flow administration.
Severe respiratory distress, poor capilary refill or other indications of poor oxygenation.
Unresponsive patient.
Obstetric patients with known or suspected complications.
CPAP administration.
Contraindications:
None (unless specifically instructed by a physician.)
Precautions:
This guideline refers to spontaneously breathing and adequately ventilating patients only.
High concentration Oxygen in some cases (emphysema) may depress the respiratory drive; be prepared to assist
ventilations, but don’t allow patients to become severely hypoxic for fear of respiratory arrest.
Many studies have shown worse outcome with excess oxygen administration (COPD, MI, CVA, resuscitated cardiac arrest and
newborns).
Agitation or restlessness can be a sign of hypoxia.
Do not use in the presence of open flames.
In the treatment for anxiety; hyperventilation should be treated with reassurance and coaching to slow breathing. If the
possibility of another underlying cause exists (i.e. pulmonary embolus, asthma, heart attack) then the patient should be
treated with oxygen. DO NOT treat any patient by having them breathe into a paper
bag or Oxygen mask that is not supplied with Oxygen.
Adverse Reactions / Side Effects:
Non-humidified oxygen can dry mucous membranes.
Administration:
Deliver low concentrations via nasal cannula @ 1-6 L/min.
Deliver high concentrations via non-rebreather mask or BVM @ 10-15 L/min.
Obtain and document pulse oximetry readings before and during oxygen therapy.
Titrate flow rate DOWN to minimum flow rate necessary to achieve protocol specific target level and DISCONTINUE if
able once target SpO2 achieved. (Except Carbon Monoxide poisoning, maintain high flow).
SPECIAL NOTES: Always treat your patient based on signs and symptoms. Do not rely on the pulse Oximetry reading to determine
appropriate care. If Oximetry is unavailable, patients should receive high concentration oxygen based on assessment
indications.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Equipment & Procedures
Guideline Number - 4025
BAG VALVE MASK (BVM)
4025 - BAG VALVE MASK (BVM)
Bag-Valve-Mask (BVM)-consists of a self-inflating bag, one-way valve, face mask, and oxygen reservoir. The most difficult
part of delivering BVM ventilation’s is obtaining an adequate face mask seal. Therefore it is strongly recommended that BVM
artificial ventilation be performed by two rescuers.
Perform BVM Ventialation as per below -
Open the patient’s airway using the HEAD-TILT, CHIN-LIFT TECHNIQUE. Suction and insert an airway adjunct
(oral or nasal).
Select the correct bag size.
Kneel at the patient’s head. Position thumbs over the top half of the mask, index and middle fingers over the bottom half.
Place the apex or top of the triangular mask over the bridge of the patient’s nose, then lower the mask over the mouth and upper
chin. If the mask has a large, round cuff surrounding a ventilation port, center the port over the patient’s mouth.
Use ring and little fingers to bring the patient’s jaw up to the mask and maintain the head-tilt, chin-lift.
The second rescuer should connect bag to mask, if not already done. While you maintain the mask seal, the second rescuer should
squeeze the bag with one hand JUST UNTIL THE PATIENT’S CHEST RISES. If using a BVM with manometer do not exceed 30
cmH20 of pressure.
The second rescuer should release pressure on the bag and let the patient exhale passively. While this occurs the bag is refilling
from the oxygen source.
Open the patient’s airway USING THE JAW-THRUST TECHNIQUE. Suction and insert an oral airway. (May utilize the Head-Tilt
Chin-lift if the airway cannot be opened by the jaw-thrust technique.)
Select the correct BVM size.
Kneel at the patient’s head. Place thumbs over the nose portion of the mask and place your index and middle fingers over the
portion of the mask that covers the mouth.
Use your ring and little fingers to bring the jaw upward, toward the mask, WITHOUT TILTING THE HEAD
OR NECK.
The second rescuer should squeeze the bag to ventilate the patient as described above for the No Trauma patient.
NOTE: If the airway cannot be opened by the JAW-THRUST TECHNIQUE, revert to the
HEAD-TILT, CHIN-LIFT TECHNIQUE as a last resort.
Position yourself at the patient’s head and establish an open airway. Suction and insert an airway adjunct as necessary.
Select the correct BVM size. Position the mask on the face as described above.
Form a “C” around the ventilation port with thumb and index fingers. Use the middle, ring and little fingers under the patient’s
jaw to hold the jaw to the mask.
With your other hand, squeeze the bag JUST UNTIL THE PATIENT’S CHEST RISES. If using a BVM with manometer do
not exceed 30 cmH20 of pressure.
Release pressure on the bag and let the patient exhale passively. While this occurs the bag is refilling from the oxygen
source.
If the chest does not rise and fall with BVM Ventilations:
Reposition the head.
Check for escape of air around the mask and reposition fingers and mask.
Check for airway obstruction or obstruction in the BVM system.
Re-suction the patient if necessary. Insert an airway adjunct if not already done.
If none of the above methods work, use a pocket mask with a one-way valve.
When ventilating squeeze slowly and gently until you get chest rise.
Artificial ventilation of a stoma breather:
Clear any mucous plugs or secretions from the stoma.
Leave the head and neck in a neutral position, as it is unnecessary to position the airway prior to ventilation’s in a stoma
breather.
Use a pediatric size mask to establish a seal around the stoma.
Ventilate at the appropriate rate for the patient’s age.
If unable to artificially ventilate through the stoma, consider sealing the stoma and attempting artificial ventilation through
the mouth and nose.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Equipment & Procedures
Guideline Number - 4075
CPR-AED
4075 - CPR-AED
4075 - CPR-AED
CPR comes first. Determine unresponsiveness, open airway and begin CPR.
Chest compressions at a rate of 100 - 120/minute, allowing complete chest recoil by not resting any weight of the rescuer on the
patients chest.
Do not interrupt CPR except when absolutely necessary.
OPA / NPA or iGel airway required during BVM ventilation.
Ventilate at no more than 10 breaths per minute.
Compressions should be delivered continuously with ventilations interspersed every 6 seconds.
Attach ResQpod to mask or Supraglottic Airway (iGel). If applied to mask, a 2-hand seal MUST BE CONTIUOUSLY
MAINTAINED!
A pulse check may be taken during rhythm analysis as long as it does not interfere with the analysis.
All contact with patient must be avoided during delivery of shock(s).
Automated external defibrillation using a device with Pediatric pads and cables is preferred for children less than 8 years
old.
Preferred placement of AED pads is right upper chest and left lower chest wall.
Call for ALS backup immediately.
Preparation for transport of patient should begin staffing allows.
Assuming no onscene ALS, the patient should be transported by the time one of the following occurs:
The patient regains a pulse.
Three shocks are delivered.
The machine gives three consecutive messages (separated by two minute of CPR) that no shock is advised.
If automated external defibrillators can not analyze rhythm properly when emergency vehicle is in motion, stop vehicle.
OPERATIONAL STEPS -
Stop CPR if in progress.
Verify pulselessness and apnea.
Resume CPR while preparing for AED use as soon as possible.
Turn on defibrillator power and attach device.
Stop CPR.
Clear patient.
Initiate analysis of rhythm. If AED advises shock:
Deliver shock.
Perform 2 minutes of CPR.
Insert Supraglottic Airway (iGel) and attach ResQPOD if not already in place.
Check Pulse and Analyze Rhythm.
If machine advises shock, deliver second shock.
If no pulse perform 2 minutes of CPR.
Check Pulse and Analyze Rhythm.
If machine advises shock, deliver third shock.
Perform 2 minutes of CPR.
Check pulse and Analyze Rhythm.
If pulse returns, check breathing and ensure adequate ventilation and remove ResQPod.
If no pulse:
Resume CPR for two minutes.
Repeat steps 6 - 8.
If, after any rhythm analysis, the machine advises no shock, check pulse.
If pulse is present, check breathing, and ensure adequate ventilation.
If no pulse, resume CPR for two minutes and repeat rhythm analysis. If AED advises shock, repeat steps 6 - 8.
If no shock continues to be advised, resume CPR for additional 2 minutes and analyze rhythm again.
If no shock continues to be advised, resume CPR and transport.
Verify pulselessness and apnea.
Turn on defibrillator power and attach device while beginning narrative.
Clear patient.
Initiate analysis of rhythm. If AED advises shock:
Deliver shock.
Perform 2 minutes of CPR
Hands-Only (compression only) CPR is acceptable if airway equipment or face mask are not available.
Check pulse and Analyze Rhythm.
If machine advises shock, deliver second shock.
Perform 2 minutes of CPR.
Check Pulse and Analyze Rhythm.
If machine advises shock, deliver third shock.
Perform 2 minutes of CPR.
Check pulse and Analyze Rhythm.
If pulse returns, check breathing and ensure adequate ventilation.
If no pulse returns continue CPR until ALS arrives.
If, after any rhythm analysis, the machine advises no shock, check pulse.
If pulse is present, check breathing, and ensure adequate ventilation.
If no pulse, resume CPR for two minutes and repeat rhythm analysis. If AED advises shock, repeat steps 4 and 5.
If no shock continues to be advised, resume CPR for additional 2 minute and analyze rhythm again.
If no shock continues to be advised, resume CPR until help arrives.
In the event that return of spontaneous circulation occurs the initial objectives of post-resuscitation care are to:
Transport the victim of out-of-hospital cardiac arrest hospital to the nearest emergency department (ED).
Try to identify the precipitating causes of the arrest (Hs and Ts).
Externally cool the patient by placing chemical cold packs in the patient’s arm pits, groin and on the neck (carotid
arteries).
Airway:
Ensure Supraglottic Airway is properly secured and patient is easy to ventilate.
Assess pulse Oximetry continuously.
Maintain end-tidal CO2 between 30-40 mmHg. If less than 30 slow ventilation rate. If greater than 40 increase
ventilation rate.
Circulation:
Assess presence of pulses and attempt to obtain blood pressure.
If hypertensive monitor frequently.
Neurological:
Assess AVPU.
Metabolic:
Obtain blood glucose and administer Glucagon if less than 70.
Temperature Control:
Do not attempt to warm patient unless hypothermia is the suspected cause of the arrest.
Apply Ice Packs to axila, groin, and neck.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Equipment & Procedures
Guideline Number - 4100
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP)
4100 - CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP)
Continuous Positive Airway Pressure has been shown to rapidly improve vital signs, gas exchange, and the work of breathing,
decrease the sense of dyspnea, and decrease the need for endotracheal intubation in patients who suffer respiratory distress
from asthma, COPD, pulmonary edema, CHF, and pneumonia. In patients with CHF, CPAP improves hemodynamics by reducing preload
and afterload.
Any patient who is complaining of shortness of breath for reasons other than trauma and:
Is awake and able to follow commands.
Is over 12 years old and is able to fit the CPAP mask.
Has the ability to maintain an open airway.
A respiratory rate greater than 25 breaths per minute.
Has a systolic blood pressure above 100mmHg.
Uses accessory muscles during respirations.
Sign and Symptoms consistent with COPD, pulmonary edema/CHF.
Patient is in respiratory or cardiac arrest.
Patients suspected of having a pneumothorax (unequal breath sounds).
Patients at risk for vomiting.
Patient has a tracheostomy.
Use care if patient:
Has impaired mental status and is not able to cooperate with the procedure.
Has failed at past attempts at noninvasive ventilation.
Has active upper GI bleeding or history of recent gastric surgery.
Complains of nausea or vomiting.
Has inadequate respiratory effort.
Has excessive secretions.
Has a facial deformity that prevents the use of CPAP.
If utilizing CPAP with a portable O2 tank, pay particular attention to oxygen levels as small tanks can deplete
quickly. When in the ambulance it is preferable to utilize the on-board oxygen.
EXPLAIN THE PROCEDURE TO THE PATIENT.
Ensure adequate oxygen supply to ventilation device (100%).
Place the patient on continuous pulse Oximetry.
Place the delivery device over the mouth and nose.
Secure the mask with provided straps or other provided devices.
Use in CPAP MODE only at 11 - 12 cm H2O (15 LPM).
Check for air leaks.
Monitor and document the patient’s respiratory response to treatment.
Monitor vital signs at least every 5 minutes. CPAP can cause BP to drop.
Monitor LOC closely. Worsening LOC indicates impending respiratory arrest. Be prepared to discontinue CPAP and assist
ventilations.
Monitor and document the patient’s respiratory response to treatment.
Continue to coach patient to keep mask in place and readjust as needed.
If respiratory status deteriorates, remove device and assist ventilations as needed.
CPAP therapy needs to be continuous and should not be removed unless the patient can not tolerate the mask or experiences
continued or worsening respiratory failure.
Consider assisting ventilations manually if the patient is removed from CPAP therapy.
CPAP may be discontinued if patient improves dramatically but be prepared to reinstitute CPAP is needed.
CPAP should not be used in children under 12 years of age.
Bronchodilator nebulization may be placed in-line with CPAP circuit.
Do not remove CPAP until hospital therapy is ready to be placed on patient.
Most patients will improve in 5-10 minutes. If no improvement within this time, consider assisting ventilations manually.
Watch patient for gastric distention. Be prepared for vomiting.
CPAP does not violate DNR Order.
Request ALS intercept if patient condition does not improve.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Equipment & Procedures
Guideline Number - 4140
GLUCOMETER
4140 - GLUCOMETER
Blood glucose determination is essential in managing a patient with a suspected diabetic problem. If the patient’s blood sugar
is below “normal” and are showing signs and symptoms of a hypoglycemic reaction, RMC EMTs may be able to administer medication to
provide relief of the symptoms.
All glucometers MUST be tested and documented by approved laboratory methods with each “rig” check (but at least once per week).
When confronted with a patient presenting with S&S of hypoglycemia, the EMT should:
Obtain a complete set of Vital Signs; include O2 saturation if available.
Check Blood Glucose and place lancet in an approved sharps container.
If Blood Glucose is greater than 70 mg/dL and the patient has an altered mental status, confirm ALS is enroute and monitor
the A, B, C’s.
If hypoglycemic (< 70 mg/dL) and awake (A or V on AVPU) with the ability to maintain their airway; administer oral glucose
consistent with RMC BLS Protocol. Repeat Vital Signs and AVPU after 5 minutes (including a repeat glucose check).
If completely alert and oriented, request MEDICAL CONTROL approval to cancel
ALS.
Continue on going assessment consistent with current RMC BLS Protocols.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Equipment & Procedures
Guideline Number - 4170
PERIPHERAL INTRAVENOUS ACCESS
4170 - PERIPHERAL INTRAVENOUS ACCESS
(OPTIONAL) Requires EMSRB Variance Approval per Minnesota Rules 4690.8300 SPECIFIC VARIANCES Subpart 7
Assess indications and explain procedure to patient/family.
Indications:
Administration of medication, fluids or nutrition.
Contraindications:
Thrombosis (blood clot in extremity be accessed).
Phlebitis (vein infection) or skin infection in extremity.
Arm on side of mastectomy, dialysis shunt or distal to area of trauma.
Equipment:
Alcohol swab.
Tourniquet.
Appropriate size catheter.
Tape or occlusive dressing.
IV fluids and IV tubing or saline lock.
Site selection will depend on many factors including: Patient comfort, accessibility, urgency of IV access, intended use
and patient age. In general, more distal sites should be selected first. This allows use of a more proximal site if initial
attempt is unsuccessful. Acceptable sites include: dorsal hand, forearm, antecubital (higher likelihood of position related flow
obstruction), foot, lower leg and scalp in children.
Apply a tourniquet proximal under tension.
Consider venous dilation; active or passive pumping of an extremity, or gravity.
Clean skin with alcohol swab.
Stabilize skin by taught traction distally with the non-dominant hand.
Puncture skin at a 30o angle, bevel up, just over or parallel to the vein. Once blood is seen in the flash
chamber, the catheter is advanced over the needle.
Remove needle, dispose of in sharps container.
Connect IV tubing or saline lock.
Open IV flow to ensure that IV is patent and that no infiltration has occurred.
Adjust flow rate as appropriate.
Apply tape or dressing. Additional dressing or tape may be used to prevent accidental removal.
Prevention and Management
4170 - IV Access
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Equipment & Procedures
Guideline Number - 4200.10
i-gel AIRWAY
4200.10 - i-gel AIRWAY
Indications :
Patient is unconscious and unable to protect own airway.
No apparent gag reflex.
Contraindications :
Patient with an intact gag reflex.
Ingestion of caustic substance(s).
Don protective eyewear, mask and gloves.
Ventilate patient with oral/nasal airways and BVM with 100% supplemental oxygen during preparation of i-gel.
Select appropriate size (Sized by ideal body weight):
#1 – for patients 2 kg - 5 kg (4 lbs - 11 lbs)
#1.5 – for patients 5 kg - 12 kg (11 lbs - 26 lbs)
#2 – for patients 10 kg - 25 kg (22 lbs - 55 lbs)
#2.5 - for patients 25 kg - 35 kg (55 lbs - 77 lbs)
#3 - for patients 30 kg - 60 kg (60 lbs - 132 lbs)
#4 – for patients 50 kg - 90 kg (110 lbs - 198 lbs)
#5 – for patients 90+ kg (198+ lbs.)
Open the i-gel package and on flat surface take out the protective cradle containing the device.
Remove the i-gel and transfer to the palm of the same hand that is holding the protective cradle, supporting the device
between the thumb and index finger.
Place a small bolus of a water based lubricant, such as K-Y Jelly, onto the middle of the smooth surface of the protective
cradle in preparation for lubrication.
Grasp the i-gel with the opposite (free) hand along the integral bite block and lubricate the back, sides and front of the
cuff with a thin layer of lubricant.
Grasp the lubricated i-gel firmly along the integral bite block. Position the device so that the i-gel cuff outlet is facing
towards the chin of the patient. The patient should be in the "sniffing" postion with head extended and neck flexed unless
you suspect c-spine injury, then place in a neutral in-line position. The chin should be gently pressed down before
proceeding.
Introduce the leading soft tip into the mouth of the patient in a direction towards the hard palate.
Glide the device downwards and backwards along the hard palate with a continuous but gentle push until a definitive
resistance is felt.
The tip of the airway should be located into the upper esophageal opening and the cuff should be located against the laryngeal
framework. The incisors should be resting on the integral bite-block.
Attach the manual resuscitator bag to the i-gel Airway device.
Confirm correct placement by listening for breath sounds, observing the chest rise and fall.
Secure the i-gel Airway device with tape or with the supplied head strap. Consider use of C-collar to restrict head
movement.
If using i-gel Airway device, consider decompressing the stomach by inserting a nasogastric tube through the gastric outlet
on the airway.
Removal of the airway is indicated -
IF the patient has a return of gag reflex AND ability to protect own airway,
OR
If ventilation is inadequate.
Don protective eyewear, mask and gloves.
Vomiting is likely, have suction ready with Yankauer tip.
If not contraindicated by suspected spinal injury, turn the patient to the side.
Carefully remove the i-gel Airway device staying alert for vomiting.
Oxygenate and ventilate as needed.
Sometimes a feel of "give-way" is felt before the end point resistance is met. This is due to the passage of the bowl of
the i-gel through the faucial pillars. It is important to continue to insert the device until a definitive resistance is felt.
Once definitive resistance is met and the teeth are located on the integral bite-block, do not repeatedly push i-gel down or
apply excessive force during insertion.
If there is early resistance during insertion -
A "jaw-thrust" (above) or "Insertion with Deep Rotation" (right) is
recommended.
It is not necessary to insert fingers or thumbs into the patients mouth during the process of inserting the device.
No more than three attempts in one patient should be attempted.
i-gel Airway Chart
from "IS6.3_igel_UK_issue_11_web.pdf"
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Equipment & Procedures
Guideline Number - 4275
PULSE OXIMETRY
4275 - PULSE OXIMETRY
Respiratory distress / complaints.
Cardiac problems.
Multiple system trauma.
Poor color.
Patients requiring use of airway adjuncts and / or assisted ventilation’s.
Suspected shock.
Altered level of consciousness.
NOTE: Never withhold Oxygen from a symptomatic patient regardless of the pulse Oximetry reading.
Patients with hemoglobin disorders suchas CO poisoning, anemia, and methemoglobinemia may give artificially high saO2
readings. Readings in such patients should be interpreted with extreme caution.
Pulse Oximetry readings may be difficult to obtain in states of low perfusion.
PROCEDURE FOR PATIENTS WITH SaO2 < 90% OR FALLING SaO2:
Check airway and manage as indicated.
Increase oxygen delivery (increase liter flow) and / or assist ventilation.
Check pulse Oximetry device placement. Possible causes of inaccurate readings include:
Excessive movement, ambient light or temperature.
Moisture in the sensor or sensor not at heart level.
Cold, blue fingertips (do NOT use thumbs).
Sensor placed on same arm blood pressure is being obtained on.
Improperly attached sensor (look for consistent flashing green light).
Incorrect sensor for patient (do NOT use on neonates or infants).
Poor patient perfusion (light should blink green and heart rate digital reading should be the same as the patients
radial pulse when taken).
Special probes may be required to obtain readings in pediatric patients.
Best probe site in adults is usually the middle finger tip with nail polish removed.
Attempt to obtain and document pulse Oximetry readings before and during oxygen therapy.
The use of pulse Oximetry as a vital sign is encouraged, as the oximeter may be helpful in detecting hypoxia not evidenced by
signs or symptoms.
Sensor sites (fingertips) must be checked periodically to determine sensor positioning, skin sensitivity and circulation (pink,
warm, warm, capillary refill less than 2 seconds).
Clean Oximeter with disinfectant.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Equipment & Procedures
Guideline Number - 4300
ResQPOD
4300 - ResQPOD
The ResQPOD Circulatory Enhancer provides a small but important amount of resistance when the patient inhales through the device.
This resistance increases blood flow back to the heart which increases the preload of the heart.
Indications:
Cardiac Arrest (ResQPOD)
Contraindications:
Do not use in patient < 12 y/o or under 100 lbs.
Procedure:
Select airway adjunct (OPA/NPA, King Airway, iGel).
Turn timing lights on. The timing lights indicate when a ventilation should be administered.
Continue CPR allowing complete chest re-coil after each compression.
Assure proper ventilation rates of 8-10/min.
Place ResQPOD between adjunct and bag-valve mask with supplemental Oxygen and ensure the mask has a continuous tight seal.
Ensure King Airway or iGel is properly placed and secured with a mechanical tube holder.
Use caution so additional weight of ResQPOD does not move the King Airway or iGel.
Document time ResQPOD is placed in circuit and any changes in skin color.
If ResQPOD fills with blood / emesis / fluid, remove and shake the fluid out. Re-apply and continue ventilations
Remove if Return of Spontaneous Circulation (ROSC) if achieved.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Equipment & Procedures
Guideline Number - 4325
"COMBAT-TYPE" TOURNIQUET USE
4325 - "COMBAT-TYPE" TOURNIQUET USE
Background
Conventional methods for controlling severe hemorrhage include direct pressure, pressure dressings and elevation.
These techniques tend to require constant pressure using both hands, thus consuming one care provider. Recent military data have
demonstrated excellent bleeding control with acceptable limb salvage rates using combat application tourniquets (CAT). These devices
also allow for continued care of other injuries and patients. Obvious exsanguinating hemorrhage should be rapidly control prior
to any other emergent interventions.
Indications
Failure to stop bleeding with direct pressure or pressure dressing.
Injury does not allow for hemorrhage control with pressure.
Significant extremity hemorrhage in the face of any or all:
Need for airway management
Need for ventilator support
Circulatory shock
Need for other emergent interventions or assessment
Bleeding from multiple locations
Impaled foreign body with ongoing extremity bleeding.
Under fire or other dangerous situation for responding caregivers.
Total darkness or other adverse environmental factors.
Mass casualty, number of casualties exceeds ability to provide optimal care.
Protocol
For severe bleeding associated with limb amputation or signs of shock with other exsanguinating hemorrhage,
skip to D (apply tourniquet)
Attempt to control bleeding with direct pressure or application of pressure dressing.
If profuse bleeding persists after 5 min or unable to maintain pressure due to other patient care needs, apply tourniquet.
Apply to appropriate above bleeding site on humerus or femur area per manufacturer’s instructions.
Tighten windlass until bleeding stops and loss of distal pulse.
Secure windlass and tighten safety screw (if applicable).
Write time of application on strap time tag (or on skin above tourniquet if no tag).
Notify dispatch at the time of application for back-up record of time.
Specify site and patient ID if multiple patients or sites.
Do not cover tourniquet unless risk of cold or environmental injury.
At 30 min of tourniquet time, reassess for removal:
If shock, clinically unstable, limited personnel / resources or amputated extremity,
DO NOT remove, otherwise;
Apply pressure dressing and loosen tourniquet (leave in place).
If re-bleeding occurs tighten to stop bleeding.
If bleeding site is not amenable to tourniquet placement (e.g axilla or groin) may apply deep wound packing with
hemostatic or standard gauze packing.
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Appendix
Guideline Number - 5050
ACCEPTABLE ABBREVIATIONS
5050 - ACCEPTABLE ABBREVIATIONS
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Reference Charts
Guideline Number - 5170
CINCINNATI STROKE SCALE
5170 - CINCINNATI STROKE SCALE
5170 - Cincinnati Stroke Scale
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Reference Charts
Guideline Number - 5200
GLASCOW COMA SCALE
5200 - GLASCOW COMA SCALE
5200 - Glascow Coma Scale
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Reference Charts
Guideline Number - 5250
SELECTIVE SPINE PRECAUTIONS
5250 - SELECTIVE SPINE PRECAUTIONS
Stage 1 Selective Spinal Precautions
Stage 2 Selective Spinal Precautions
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Do Not Resuscitate
Guideline Number - 5325
DO NOT RESUSCITATE
5325 - DO NOT RESUSCITATE
5325 - Do Not Resuscitate
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Do Not Resuscitate
Guideline Number - 5350
DNR FORM
5350 - DNR FORM
5350 - DNR Form
5350 - DNR Form
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Skills Verification Forms
Guideline Number - 5500
Medical Director Skill Assessment Verification
5500 - Medical Director Skill Assessment Verification
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Skills Verification Forms
Guideline Number - 5550
Medical Director Variance Medication Annual Skill Verification
5500 - Medical Director Variance Medication Annual Skill Verification
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Skills Verification Forms
Guideline Number - 5600
Annual Medical Director Approval of Specific Procedures for Basic Life Support Services
5600 - Annual Medical Director Approval of Specific Procedures for Basic
Life Support Services
rev. 2 April 2019
rev. 2 April 2019
Ridgeview Ambulance Protocols
Skills Verification Forms
Guideline Number - 5650
Medical Director Skill Assessment Verification - Designee
5650 - Medical Director Skill Assessment Verification - Designee
The Hennepin County Emergency Medical Services (EMS) system refers to a dedicated group of professionals
working together to provide emergency medical services to patients and communities within Hennepin County.
The EMS system is a dynamic mix of private and public providers including:
Ambulance Services
First Responders (Public Safety and Fire Services)
Dispatchers
Medical Control Hospital Physicians
Acute and Tertiary Care Emergency Facilities
County Public Health Staff
The Hennepin County Board of Commissioners makes general policy decisions affecting the EMS system in
response to recommendations from the Emergency Medical Services Advisory Council. The Hennepin County EMS
Planning and Regulatory Unit (EMS Unit) is a division of the Human Services and Public Health Department and
provides planning support and regulatory oversight for the county’s EMS system and assures coordinated
emergency response to 911 calls.
The Emergency Medical Services Council was established in 1976 to recommend to the Hennepin County Board of
Commissioners and other appropriate authorities activities and processes necessary for the coordination and
improvement of prehospital emergency services within Hennepin County. Committees of the council include:
Executive Committee
Operations Committee
Quality Committee
Medical Standards Committee
Ambulance Medical Directors Subcommittee
Ambulance Service Personnel Subcommittee
Five Advanced Life Support (ALS) ambulance services provide emergency medical care to Hennepin County
residents. The Minnesota Emergency Medical Services Regulatory Board (EMSRB) designates Primary Service
Areas (PSAs) for ambulance services operation within the state of Minnesota. The five services which are
authorized by the EMSRB to operate within Hennepin County are:
Allina Health EMS
Edina Fire Department
Hennepin EMS
North Memorial Ambulance Service
Ridgeview Ambulance Service
ALS protocols and guidelines for Hennepin County’s EMS system are reviewed and re-issued on an on-going basis. New
protocol proposals and/or protocol revision proposals are reviewed by the Ambulance Service Personnel Subcommittee,
the Ambulance Medical Directors Subcommittee and the Medical Standards Committee. The Emergency Medical Services
Advisory Council is the final reviewing authority for protocol changes.
Individuals interested in developing new ALS protocols and/or guidelines or interested in revising current ALS
protocols and/or guidelines may request a Protocol Revision Form from the public health EMS Unit at
chd.ems@hennepin.us, by calling 612-348-6001, or
by visiting our website at www.hennepin.us/ems.
AUTHORITY
Each of the ambulance services operating a Primary Service Area (PSA) within
Hennepin County has an ambulance service medical director. Per MN Statute 144E.265,
Subd. 2, "Responsibilities of the medical director shall include, but are not limited
to:
Approving standards for education and orientation of personnel that impact patient care;
Approving standards for purchasing equipment and supplies that impact patient care;
Establishing standing orders for prehospital care;
Approving written triage, treatment and transportation guidelines for adult adn pediatric patients;
Participating in the development and operation of continuous quality improvement programs including, but not
limited to:
Case Review
Resolution of Patient Complaints
Establishing procedures for the administration of drugs;
Maintaining the quality of care according to the standards and procedures established under clauses (1) to (6)."
The policies and protocols in this document represent the collective medical expertise and authority of the medical directors
for the five ALS ambulance services operating PSAs within Hennepin County. If any conflict exists between a service specific
policy or protocol and a system policy or protocol, paramedics shall follow their service policy.
Created Date: Unknown
Created Date: Unknown
Ridgeview Ambulance Protocols
Guidelines
Protocol 2001
GUIDELINES
2001 - GUIDELINES
These medical protocols are intended for use while working under the license of an Ambulance Medical Director for an
ambulance service with a Primary Service Area (PSA) in Hennepin County.
Remember: courtesy to the patient, the patient's family and other emergency care personnel is of utmost importance.
A Patient Care Report (PCR) form must be completed on all patients and a copy left with the patient at the hospital. See
www.hennepin.us/ems for the Required Documentation Policy. Specific
prehospital care information must also be recorded on all patientccontacts as part of the MNStar requirements and Hennepin County
System Data Collection Program.
All equipment appropriate to the nature of the call for assistance, treatment and transport should be taken to the site
of the patient at the time of the initial patient contact.
In all circumstances, physicians have latitude in the care they give and may deviate from these Medical Protocols if it
is felt such deviation is in the best interest of the patient. Nothing in these protocols shall be interpreted as to limit
the range of treatment modalities available to meical control physicians to utilize, other than the modalities and the
medications used must be consistent with the paramedic's training.
The specific conditions listed for treatment in this document, although frequently stated as medical diagnoses, are
operational diagnoses to guide the paramedic in initiating appropriate treatment. This document is to be used as consultive
material in striving for optimal patient care. It is recognized that specific procedures and/or treatments may be modified
depending on the circumstances of a particular case. Also, a medical control physician when consulted will either concur or
further evaluate the paramedic's clinical findings and suggest an alternate diagnosis and treatment.
Revision Date: 7 June 2012
Revision Date: 7 June 2012
Ridgeview Ambulance Protocols
Guidelines
Protocol 2010
CRITICAL INCIDENT STRESS DEBRIEFING (CISD)
2010 - CRITICAL INCIDENT STRESS DEBRIEFING (CISD)
Paramedics and other EMS personnel are encouraged to fammiliarize themselves with the causes and contributing
factors of critical incident and cumulative stress, and learn to recognize the normal stress reactions that
can develop from providing emergency medical services.
A "Metro CISM Team" is available to paramedics and other EMS personnel. The program consists of mental health
professionals, chaplains and trained peer support personnel who develop stress reduction activities, provide
training, conduct debriefings and assist EMS personnel in locating available resources. The team will provide
voluntary and confidential assistance to those wanting to discuss conflicts or feelings concerning their work
or how their work affects their personal lives.
Deactivate an ICD only after consultation with a medical control physician.
Establish on ECG that the ICD is inappropriately discharging in the presence of a non-VT/VF rhythm.
To deactivate the ICD -
Locate the pulse generator on the patient.
Place a donut magnet over the generator.
Depending on the ICD brand, you may or may not hear a high-pitched tone.
Secure the magnet in place with adhesive tape.
The magnet will inhibit further arrhythmia detection and treatment by the ICD.
Revision Date: 11 October 2012
Revision Date: 11 October 2012
Ridgeview Ambulance Protocols
Guidelines
Protocol 2030
LIMITING RESUSCITATION MEASURES AND DNR
2030 - LIMITING RESUSCITATION MEASURES AND DNR
Cardiopulmonary Resuscitation (CPR) will be promptly instituted for all patients found in cardiac arrest
unless reliable criteria for the determination of death are present, or if a valid DNR or No CPR order
exists.
Reliable criteria for the determination of death include:
Lividity
Rigor
Obviously fatal trauma
Absence of vital signs in a trauma victom upon arrival of EMS personnel despite a patent airway
Do Not Resuscitate (DNR, No CPR) orders are issued by a patient's physician to prevent rescuers from
initiating resuscitative measures in the event of a cardiopulmonary arrest. Patients with DNR orders
may receive vigorous medical support, including all interventions specified in the ALS Medical Protocols,
up to the point of cardiopulmonary arrest.
In the healthcare facility -
A DNR order is valid if it is written in the order section of the patient
chart (or on a transfer form) and is signed by a physician, registered nurse practitioner or physician
assistant acting under physician authority. Copies of the order are valid.
A DNR form (See 9050 - Do Not Resuscitate (DNR) Guidelines
- section D for examples for DNR forms you may encounter,) must be signed by the patient or proxy, the
physician and a witness in order to be valid. No validation stamp or notarization is necessary and a
legible copy is acceptable.
If possible, the DNR order or copy should accompany the patient to the hospital. Pertinent documentation
should be included on the ambulance report form for the run. In the event of confusion, questions
regarding the DNR order, or if you are being directed by family members to perform actions in opposition to those listed on
DNR order, resuscitation should be initiated and a medical control physician should be
consulted.
Living wills should not be interpreted at the scene, but conveyed to the physicians in the receiving
emergency department.
A medical control physician should be contacted as specified in these protocols.
Whenever possible, medical control should be obtained from the destination hospital requested by the patient.
If the destination hospital is unable to provide medical control, paramedics may contact their service's default
medical control hospital. Default medial control hospitals for each service are:
Allina Health EMS - Abbott Northwestern Hospital
Edina Fire Department - Fairview Southdale Hosital
Hennepin EMS - Hennepin County Medical Center
North Memorial Ambulance - North Memorial Medical Center
Ridgeview Ambulance -
Ridgeview Medical Center - Waconia
Two Twelve Medical Center - Chaska
Except for load-and-go situations with short transport times, any such delay in establishing medical control will
be explained in a System Incident Report submitted by the paramedics to their medical director and to the Hennepin
County Human Services and Public Health Department. This policy in no way precludes establishment of medical control
at any time during the run to obtain physician advice or assistance.
In the occurance of communication failure, paramedics may perform those orders outlined in the ALS Medical Protocols
under "After Obtaining Verbal Orders" for patients with life-threatening or potentially life-threatening conditions.
Initiation and performance of these orders must be in accordance with the paramedic's training and must be carried out
as written in these Medical Protocols.
Any instance of communications failure where procedures are carried out without a physician's verbal order must be
reported in a System Incident Report within 48 hours to the paramedic's medical director and to the Hennepin County
Human Services and Public Health Department.
Revision Date: 11 October 2011
Revision Date: 11 October 2011
Ridgeview Ambulance Protocols
Guidelines
Protocol 2050
MULTIPLE CASUALTY INCIDENTS (MCI)
2050 - MULTIPLE CASUALTY INCIDENTS (MCI)
In special incidents with potental for multiple casualties, resources for the EMS system may be
temporarily overwhelmed or extended to their limits.
A system plan for EMS response to Multiple Casualty Incidents (MCIs) establishes a framework for coordinating resources
during incidents requiring various ambulance providers, hospitals and public safety agencies to work together to optimize
patient care and transportation with the given resources of the community. The goals of the system plan are to:
Recognize and maintain operations of ambulance providers, hospitals, and other agencies as close to normal as possible.
Utilize the incident command structure to allow flexibility for effective response to a variety of hazards most likely
to occur within the County, including natural disaster, hazardous material exposure, urban fire, air crash, civil unrest
or any incident with actual or potential multiple casualties.
Set system standards to aid individual agencies when developing policies and procedures.
As rapidly as possible transport patients to appropriate hospital(s).
Ambulance services operating a Primary Service Area (PSA) in Hennepin County shall follow the regional Incident Response
Plan (IRP) during a Major Incident or Multiple Casualty Incident (MCI). Please see the latest version of the IRP for the
definition of a Major Incident or Multiple Casualty Incident (MCI). Contact the Metro Region EMS System office for copies.
Revision Date: 13 October 2011
Revision Date: 13 October 2011
Ridgeview Ambulance Protocols
Guidelines
Protocol 2060
OXYGEN THERAPY - GENERAL GUIDELINE
2060 - OXYGEN THERAPY - GENERAL GUIDELINE
Oxygen therapy should be administered when indicated by specific protocol.
When an EMS provider believes the patient will improve with oxygen therapy the following guidelines are applicable:
For suspected smoke / CO inhalation, pneumothorax or sickle cell crisis, initiate high flow oxygen (≥ 10 lpm) via
non-rebreather mask or BVM with appropriate airway management.
Titrate to maintain goal SpO2 of
100%.
For critically ill or unconscious patients with suspected hypoxia, initiate high flow oxygen (≥ 10 lpm) via non-rebreather
mask or BVM with appropriate airway management.
Titrate down to MAXIMUM SpO2 of 96% (Discontinue for
SpO2 ≥ 97%)
Altered Mental status or unconscious from suspect head injury. Initiate high flow oxygen (≥ 10 lpm) via non-rebreather
mask or BVM with appropriate airway management.
May titrate down to MAXIMUM SpO2 of 96%
(Discontinue for SpO2 ≥ 97%)
For patients with STEMI DO NOT initiate oxygen therapy if SpO2 > 92%
For patients with CVA DO NOT initiate oxygen therapy if SpO2 > 94%
For patients at risk for hypercapnic respiratory failure (COPD with chronic O2 use), use minimum flow necessary to
achieve target SpO2 of 90%.
For all other patients, use minimum flow necessary to achieve MAXIMUM SpO2 of 96% (Discontinue for
SpO2 ≥ 97%)
For pediatrics, if the patient is agitated use high flow blow-by O2.
To provide guidance for EMS personnel on the safe and effective administration of medications to geriatric
patients (age 65 and older), considering age-related physiological changes and increased susceptibility to adverse effects.
General Considerations:
Geriatric patients are at increased risk for polypharmacy, drug interactions, and altered pharmacokinetics.
Age-related changes, such as reduced renal and hepatic function, can affect drug metabolism and excretion.
Increased sensitivity to certain medications (e.g., benzodiazepines, opioids, anticoagulants) necessitates caution.
Assessment Prior to Medication Administration:
Obtain a thorough medication history, including prescription and over-the-counter supplements.
Assess for signs of altered drug metabolism, such as confusion, dizziness, hypotension, or respiratory depression.
Medication Dosage Adjustments:
When possible, start with a lower initial dose and titrate cautiously.
For upper extremes of age and lower weight consider half initial standard adult dose (e.g. age > 85, weight < 100
lbs)
Avoid medications with strong anticholinergic properties due to increased risk of delirium and falls.
Sedatives/Benzodiazepines (droperidol, haloperidol, midazolam): Use with extreme caution due to fall and
respiratory depression risks.
Cardiovascular Medications (nitroglycerine): Monitor for exaggerated effects of nitroglycerine, consider
longer dose interval for extremes of age.
No dose adjustment needed for adenosine
Monitoring and Adverse Effects:
Monitor vital signs, mental status, and respiratory function after medication administration.
Be vigilant for signs of overdose or increased sensitivity, such as excessive sedation, hypotension, or bradycardia.
Ensure continuous cardiac and pulse oximetry monitoring when administering high-risk medications. Consider side-stream
ETCO2 monitoring.
Documentation and Communication:
Accurately document all medications given, including dose, route, and patient response.
Communicate any medication concerns or adjustments to receiving hospital staff.
Provide clear documentation of any observed adverse effects.
Special Considerations for End-of-Life Care:
Follow advance directives or physician orders for life-sustaining treatment (POLST) when applicable.
Prioritize symptom management and patient comfort.
Medical Direction and Consultation:
When in doubt, consult with online medical control for guidance on medication administration.
Revision Date: 5 February 2025
Revision Date: 5 February 2025
Ridgeview Ambulance Protocols
Guidelines
Protocol 2070
PATIENT CONSENT AND REFUSAL OF CARE
2070 - PATIENT CONSENT AND REFUSAL OF CARE
To define and establish guidelines to be followed by prehospital care providers, when a patient refuses medical evaluation,
treatment and/or transport.
Adult: Any person at or greater than the age of 18 years.
Minor: Any person who has not achieved the age of 18 years.
Minor not requireing parental consent: Any minor who -
Has an emergency condition and parent is not available.
Is or has been married.
Has given birth.
Is on active duty.
Is separated from parents (with or without their consent) and financially independent.
Is in need of pregnancy, venereal disease, or drug/alcohol related treatment (including rape.)
Request for Evaluation: A request for evaluation can be made by any individual for any reason. This request
can be made by family members, friends, first responders, law enforcement personnel, or Ridgeview Ambulance personnel.
All requests for evaluation will be honored by Ridgeview Ambulance Service and will include a complete medical
assessment appropriate to the provider's level of care.
Emergency Condition: A condition or situation (including severe pain) in which an individual had an immediate need
for medical attention, such that the absence of medical attention could place one's health (or unborn child's health)
in jeopardy.
Competent: The patient is alert and oriented and has the capacity to understand the circumstances surrounding
his/her illness or impairment and the risks associated with refusing medical evaluation, treatment and/or transport.
Refusing Care Against Medical Advice (AMA): A competent individual who is determined by pre-hospital providers to
have an emergency condition, who has been advised of this condition and the risks/possible complications of refusing
care, and still declines care.
Declining Treatment or Transportation: A competent individual (not minor) who is determined by pre-hospital providers
to not have an "emergency condition" (as defined above,) who has been offered treatment and/or transportation with
an explanation of the associated risks and benefits of this care and still declines treatment and/or transportation.
Transport Hold: An individual who is determined by law enforcement personnel or on-line medical control physician
(health officer) to be in danger of harming himself/herself or others if not immediately restrained and needs transport
to a medical facility for further evaluation.
Any competent adult or minor not requiring parental consent, has the right to determine the course of
his/her medical care, and thus is allowed to refuse care, provided the risks and potential complicaitons of refusing care have
been explained.
Any minor (except those not requiring parental consent) must have a parent or legal guardian (or responsible adult whom a
parent/legal guardian has deliberately left the minor in the care of) present to refuse medical evaluation, treatment or
transport.
Refusal of care against medical advice or declining treatment/transportation should not be considered for patients who do
not demonstrate competency. Competence may be impaired by mental illness, drug or alcohol intoxication, neurologic disease
or injury, metabolic disorders or other injury/illness. Patients who have attempted suicide, verbalized suicide intent, or
when other factors lead pre-hospital or law enforcement personnel to suspect suicidal intent, should not be regarded as
competent.
Any patient for whom a request for evaluation has been made, shall be offered medical evaluation, treatment and/or transport
by pre-hospital providers. The patient, family, friends or first responders/law enforement personnel can make this
request.
If no request for medical evaluation has been identified by first responders/law enforcement and the responding ambulance is
canceled prior to arrival the call is considered CANCELED or CANCELED EN-ROUTE.
If when the responding ambulance arrives on the scene -
Any / all involved persons should be offered evaluation by Ridgeview Ambulance Service personnel.
If EMS personnel or first responders feel a patient warrants evaluation based on mechanism and / or symptoms, or if an
evaluation is accepted, an EMS Run Report is completed for each individual who had an evaluation and the appropriate
Run Disposition selected:
Treated / Transported
Treated / No Transport (AMA)
Treated / No Transport (Per Protocol)
Any additional individuals who decline evaluation should be entered onto a refusal log.
If all involved persons decline evaluation, an EMS Run Report is completed for the event, and the event is considered
Cancelled - Cancelled on Scene (No Patient Found). Documentation within the narrative should include pertinent
information such as:
Responding ambulance findings,
Any Police or Fire personnel statements of their findings.
If a competent adult or minor who does not require parental consent, refuses medical evaluation, treatment and/or transportation
following an identified request for evaluation, pre-hospital personnel shall -
Complete a thorough medical evaluation, if consented, which will include -
Vital signs (if cooperative.)
General appearance (e.g. appears comfortable, up walking, etc.)
Mental status exam including :
Alert (eyes open, awake.)
Oriented to person, place, time.
Speech (fluent, coherent, understandable with rational thought process.)
Problem focused physical exam (if cooperative.)
Advise the individual of your preliminary medical assessment.
If an emergency condition is thought to exist -
Advise the patient of the need for immediate treatment and/or transportation and the risks and potential complications of
refusing, in the presence of a witness.
Witnesses include :
Immediate family members
Legal guardian
Power of attorney
Friends
Law enforement personnel
Ridgeview Ambulance personnel
To ensure understanding, have the patient verbalize the assessment and the risks or complications of refusal of care.
Encourage consent for care using any available means (including family, friends, etc.)
Complete the Against Medical Advice (AMA) form.
If patient refuses to sign, document this in the presence of a witness.
Contact medical control for any refusal of care Against Medical Advice or for any concerns
regarding competency or disposition.
Offer further discussion with on-line physician.
Re-offer treatment/transportation and extend that offer to any time period after leaving the scene.
Provide appropriate care and call back instructions sheet.
If an emergency condition is thought not to exist -
Offer treatment and/or transportation.
Discuss the need for further evaluation, treatment or follow-up as indicated.
Discuss the benefits of consenting to immediate treatment/transport and the risks and possible complications of declining.
Complete an EMS Run Report and have patient sign form.
If patient refuses to sign, document this in the presence of a witness.
Provide appropriate care and call back instruction sheet.
Contact medical control if any doubts concerning competency or concerns regarding disposition.
Offer treatment/trasnportation again and extend that offer to any time period after leaving the scene.
If the patient is a minor (except those not requireing parental consent) -
Determin if an emergency condition exists, if so treat/transport accordingly with implied consent -
Minors cannot refuse necessary emergency care without the approval of a parent or legal guardian.
Do not delay treatment/transport of emergency conditions in order to obtain parental consent.
If parent or guardian refuses necessary treatment, and there are concerns about neglect, or abuse, have law enforcement
respond and contact medical control for further orders.
If advised by medical control, fill out and discuss AMA form as stated in adult policy (above.)
If an emergency condition is thought not to exist and parent or guardian are not present at scene -
Attempt to contact parent or legal guardian by phone.
Discuss preliminary asessment and advise of any need for treatment/transport.
Obtain verbal consent by phone and care for accordingly.
Refusal of care cannot be given by phone. A parent, legal guardian, or apointed adult caregiver must be present on scene to
refuse care.
Document refusal per adult policy (above.)
Contact medical control for any questions or if concerns arise regarding patient disposition or
decision-making.
If a patient is refusing care against medical advice or declining treatment/trasnport and is deemed not competent to refuse
care -
Ensure scene safety and utilize law enforcement if needed.
At no time shall ambulance personnel put themselves in danger by attempting to treat or transport a patient who
refuses.
If a patient has established hospital care, (appropriate for the nature of this event) they may be transported to that
facitility. This optimizes continuity of care.
If no established care, destination hospital per county policy.
Concerns, questions or discrepancies regarding disposition and destination hospital should be discussed with medical control
physician.
If not on transport hold per law enforement and pre-hospital personnel determine the need for emergency transport hold, contact
medical control for transport hold orders.
In the case of rape, medical needs have priority over evidence collection and destination should be hospital of choice or
closest. If there are no or only minor medical concerns, then transport per county policy.
An EMS Run Report shall be completed on any patient for whom a request for evaluation has been made.
For patients who refuse care against medical advice or decline treatment and/or transportation, this report must include -
Vital signs and focused physical exam (if cooperative.)
General appearane (e.g. appears comfortable, walking, sitting, etc.)
Mental status exam, including -
Alert (eyes open, awake.)
Orientated to person, place, time.
Speech (coherent, fluent, understandable with logical thought process.)
Document specific examples of abnormalities.
The narrative portion of form should also contain -
Plan of care offered to the patient.
Reason for refusal.
Any additional means attempted to influence a patients decision (e.g. family contacted.)
Patients understanding of his/her medical condition and treatment plan.
Potential risk/complications of refusal (including death if appropriate) discussed with patient.
Any advice given to the patient (e.g. have family transport to emerency department, discuss the situation with your primary
care physician, etc.)
Patient signature or that of witness if refused.
Any discussion with on-line medical control physician.
All patients for whom a request for evaluation has been made shall be offered medical evaluation and or transport by Ridgeveiw
Ambulance personnel.
Criteria for refusing care -
An adult (18 years old or over) or a minor not requireing parental consent.
Is oriented to person, place, time and situation.
Exhibits no evidence of altered mental status or drug/alcohol ingestion that impairs judgement.
Understands the nature or their injury/illness, as well as the risks and possible consequences of refusing care.
Documentation Checklist
EXAM -
▢Complete Vital Signs
▢Mental Status -
Alert and Orientated
Speech, Behavior
Gait
▢Focused physical exam
NARRATIVE SHOULD INCLUDE -
▢Provider impression
▢Plan offered to patient.
▢Attempts to influence decision.
▢Patients verbal understanding of condition.
▢Potential risks/complications of refusal and patients verbalization of understanding
▢Any advice/forms given to patient
▢Patient signature or that of witness if refused.
▢Discussion with medical control.
Revision Date: 1 January 2020
Revision Date: 1 January 2020
Ridgeview Ambulance Protocols
Guidelines
Protocol 2080
PATIENT DISPOSITION – GENERAL GUIDELINES
2080 - PATIENT DISPOSITION – GENERAL GUIDELINES
Determination of patient disposition should be based on the following criteria:
Patient Preference – Patients should be transported to the hospital of their choice (or family's or physician's
choice). Patient preference may be overridden by:
The medical expertise of the Ambulance Medical Director,
Restriction to specific hospitals.
Medical Expertise – This authority may be represented by service specific policy, system policy, the On-Call
System Medical Director, a medical control physician, a physician on-scene who has assumed total responsibility
for the patient, or the paramedic providing patient care, (see 2160 - Physician Presence at the
Emergency Scene.) Medical expertise shall override patient preference in three
types of situations:
Patient’s preference is unavailable (e.g. closed or unreachable due to weather). See
www.hennepin.us/ems for the Hennepin County EMS System Ambulance Diversion
Policy.
Patient’s preference is inappropriate (e.g. critical trauma patient transported to a facility not capable or equipped
for the severity of the patient’s injuries.)
Patient’s preference is suboptimal for presenting condition/complaint (the following examples are not inclusive):
If unable to maintain an airway and ventilate, transport to the closest emergency department.
For patients with symptoms of severe Carbon Monoxide (CO) poisoning, consider transport to a hospital that has a hyperbaric
center.
For pregnant patients who are transported with symptoms of CO poisoning, consider transport to a hospital that has
a hyperbaric center for possible hyperbaric therapy.
Hospitals in the Twin Cities Metro area with a hyperbaric center include:
Hennepin County Medical Center (HCMC)
Signs and symptoms of severe CO exposure include:
History of loss of consciousness
Lethargy
Confusion
Disorientation
Seizures
Focal neurological deficits
Ischemic chest pain
New dysrhythmias
12 Lead ECG changes
Hypotension
Revision Date: 14 October 2010
Revision Date: 14 October 2010
Ridgeview Ambulance Protocols
Guidelines
Protocol 2100
PATIENT DISPOSITION – MAJOR BURNS
2100 - PATIENT DISPOSITION – MAJOR BURNS
For patients with major burn injuries, consider transport to a hospital that has a burn unit.
Hospitals in the Twin Cities Metro area with a burn unit include:
Ground ambulances must immediately transport patients with compromised airways (unable to maintain an airway and
ventilate) to the nearest designated trauma hospital.
If no designated trauma hospital exists within 30 minutes transport time, the patient must be transported to the
closest hospital.
In cases where a patient does not have a compromised airway, the ground ambulance must transport major trauma patients
to a level I or level II trauma hospital within thirty minutes transport time.
If no level I or level II trauma hospital exists within 30 minutes transport time, the patient must be transported
to the closest designated trauma hospital within 30 minutes transport time.
If no designated trauma hospital exists within 30 minutes transport time, the patient must be transported to the
closest hospital.
Major trauma defined as:
Amputations (proximal to mid-hand or mid-foot or with other severe trauma.
Crush injuries or prolonged entrapment/entanglement.
Blunt trauma, multisystem, with Shock
Pelvic Fractures.
Penetrating trauma to the eye(s), head, neck, chest, or abdomen, or extremity with shock.
Maxillofacial trauma, Complex: including significant tissue avulsion, unstable/displaced facial or mandible
fracture(s).
Paralysis of a limb or limbs.
Traumatic Brain Injury, Severe (GCS less than 9)
Consider transport to a level I or level II trauma center for any patient with significant trauma and any of the
following:
Severe multiple injuries (two or more systems) or severe single system injury
Cardiac or major vessel injuries resulting from blunt or penetrating trauma
Injuries with complications (e.g. shock, sepsis, respiratory failure, cardiac failure)
Severe facial injuries
Severe orthopedic injuries
Co-morbid factors (e.g. Age < 5 or > 55 years, cardiac or respiratory disease, insulin- dependent diabetes,
morbid obesity)
Evidence of traumatic brain injury and/or spinal cord injury (e.g. new paralysis)
Anticoagulation and bleeding disorders.
Age
Older Adults (risk of injury death increases after 55 years).
Children (should be triaged preferentially to pediatric-capable trauma centers).
Time sensitive extremity injury
End-stage renal disease requiring dialysis
Pregnancy > 20 weeks
Paramedic provider impression is consistent with major trauma.
Revision Date: UNKNOWN
Revision Date: UNKNOWN
Ridgeview Ambulance Protocols
Guidelines
Protocol 2115
PATIENT DISPOSITION - RECENT HOSPITALIZATION, SURGERY OR PROCEDURE
2115 - PATIENT DISPOSITION - RECENT HOSPITALIZATION, SURGERY OR PROCEDURE
Background: Patients who are seeking emergency care for problems related to recent hospitalization, surgery or
other specialized care or procedures are best served at the facility where any recent care was provided. Post-surgical or
procedural complications should be managed by the same physician, physician group or team that performed the surgery or
procedure. Seeking care at a different hospital can be detrimental if similar resources or subspecialty care is not
available. Furthermore, since the start of the COVID pandemic, hospitals and emergency departments all over the state
have been overcrowded significantly delaying or preventing transfers for definitive care.
Patients identified as having problems related to a recent hospitalization (within 72 hrs), surgery or procedure (within 1
week), shall be taken back to that facility when practical:
The Hospital is within our usual metro area facilities
If the patient requests a different facility, then transport to a hospital within the same healthcare system.
Allina (Abbott, Mercy, Unity, United, St Francis, WestHealth)
Fairview (Southdale, U of MN, St. Johns, Woodwinds, Ridges, Northland)
HealthPartners (Methodist, Regions, Lakeview)
Hennepin Healthcare (HCMC)
Mayo (Mankato, New Prague, Rochester)
North Memorial (Robbinsdale, Maple Grove
If the patient refuses the same hospital or affiliated healthcare system, contact medical control to discuss appropriate
destination.
Revision Date: 12 September 2022
Revision Date: 12 September 2022
Ridgeview Ambulance Protocols
Guidelines
Protocol 2116
PATIENT DISPOSITION – ROSC
2116 - PATIENT DISPOSITION – ROSC
Patients identified as having cardiac arrest with return of spontaneous circulation (ROSC) have a high rate of re-arrest and should
be transported to an ECMO-capable facility
U of MN East Bank
Fairview – Southdale
Abbott Northwestern
Hennepin County Medical Center
Revision Date: 23 February 2023
Revision Date: 23 February 2023
Ridgeview Ambulance Protocols
Guidelines
Protocol 2120
PATIENT DISPOSITION – STEMI
2120 - PATIENT DISPOSITION – STEMI
Patients identified with acute myocardial infarctions, as evidenced by ST elevation (STEMIs), should receive timely
transportation to a Level I Cardiac Care Facility per the EMS provider STEMI/Code AMI criteria. EMS Provider/STEMI
Code AMI inclusion criteria includes:
Patient presents with cardiac symptoms.
12-lead findings which are consistent with ST elevation greater than 1 mm in two or more contiguous leads.
QRS complex is narrower than 0.12 seconds (3 small boxes.)
If wider than 0.12, you are unable to diagnose as STEMI.
Patients identified with acute cerebral vascular accident (CVA) per the Adult Stroke (CVA) protocol
should receive timely transportation to the most appropriate designated acute stroke ready hospital, primary stroke center, or
comprehensive stroke center.
Revision Date: 14 April 2016
Revision Date: 14 April 2016
Ridgeview Ambulance Protocols
Guidelines
Protocol 2140
PATIENT DISPOSITION – TRANSPORT HOLDS
2140 - PATIENT DISPOSITION – TRANSPORT HOLDS
Paramedics may find themselves in a situation where a Transport Hold might be necessary to transport a patient
to the emergency department.
Elements of a Transport Hold (defined Minnesota Statute 253B.05 Emergency Admission Subd. 2):
A peace or health officer may take a person into custody and transport the person to a licensed physician or
treatment facility if the officer has reason to believe, either through direct observation of the person's behavior,
or upon reliable information of the person's recent behavior and knowledge of the person's past behavior or psychiatric
treatment, that the person is mentally ill or developmentally disabled and in danger of injuring self or others if not
immediately detained.
A peace or health officer or a person working under such officer’s supervision, may take a person who is believed to be
chemically dependent or is intoxicated in public into custody and transport the person to a treatment facility. 253B.05
Emergency Admission Subd. 2.
If Elements of a Transport Hold are present:
Request a Transport Hold from a Peace/Health Officer,
If the Peace/Health Officer does not provide a Transport Hold:
Contact your service’s designated home medical control hospital and ask the Medical Control Physician to speak with
the Peace/Health Officer,
If the Peace/Health Officer does not provide a Transport Hold after speaking with the Medical Control Physician:
Do not transport,
AND
Leave the patient in the care of the Peace/Health Officer.
All patients transported on a Transport Hold should be restrained during transport.
For minors, follow statute regarding Health and Welfare Holds 260C.175 subdivision 1.
Revision Date: 9 October 2014
Revision Date: 9 October 2014
Ridgeview Ambulance Protocols
Guidelines
Protocol 2150
PATIENTS WITH WEAPONS
2150 - PATIENTS WITH WEAPONS
If the patient has a weapon:
If the crew has a safety concern, call law enforcement to assist
If transporting the patient with a weapon, notify the emergency department during your pre-arrival patient care report.
Revision Date: 14 April 2016
Revision Date: 14 April 2016
Ridgeview Ambulance Protocols
Guidelines
Protocol 2160
PHYSICIAN PRESENCE AT THE EMERGENCY SCENE
2160 - PHYSICIAN PRESENCE AT THE EMERGENCY SCENE
Personal Physician -
If the patient's personal physician is present and wishes to assume responsibility for the patient's care:
The paramedic should defer to the orders of the personal physician as long as those orders are appropriate and
not in conflict with ALS Medical Protocols. Paramedics should establish medical control any time they are
uncomfortable carrying out orders from a patient's physician.
Orders given by the personal physician should be written on the EMS report form, the physician’s name documented
legibly, and signed by the physician, if possible.
System Medical Director -
If a system medical director or associate system medical director is present and wishes to assume responsibility for
the patient’s care, the paramedic should defer to the orders of the system medical director or associate system medical
director.
Medical Control Physician -
If a medical control physician is present and wishes to assume responsibility for the patient’s care, the paramedic
should defer to the orders of the medical control physician as long as those orders are appropriate and not in conflict
with ALS Medical Protocols.
Other Intervening Physician -
If any other intervening physician wishes to assume responsibility for the patient:
If medical control exists:
The intervening physician should be allowed to communicate with the medical control physician prior to the
paramedics accepting orders. If there is any disagreement between the two physicians, the paramedics will follow
the orders of the medical control physician and allow the physicians to continue their communication.
If medical control does not exist:
The paramedics should relinquish responsibility for patient management if the physician meets the following two
criteria:
can show appropriate identification (or is known to the paramedics);
agrees in advance to accompany the patient to the hospital (exception: major multiple casualty incident);
The physician’s name should be documented legibly within the PCR and, if possible, have the physician sign the EMS
report form assuming responsibility and verifying orders.
In the case of multiple intervening physicians at the scene, the paramedics should request the physicians designate
one physician to direct patient care.
Any intervening physician not wishing to assume responsibility for care and not accompanying the patient to the hospital
may be asked to assist the paramedics and/or act as a medical consultant to them and to the medical control physician.
Revision Date: 11 October 2012
Revision Date: 11 October 2012
Ridgeview Ambulance Protocols
General Adult
Protocol 3010
AIRWAY MANAGEMENT
3010 - AIRWAY MANAGEMENT
Bag Valve Mask (BVM) – Consider an oropharyngeal or nasopharyngeal airway of appropriate size on all unconscious patients
for initial airway maintenance.
Endotracheal intubation – After endotracheal intubation, tube position must be confirmed using at least two methods,
including continuous end-tidal carbon dioxide (CO2) detection and a second device or method to confirm tube
placement.
Alternate Advanced Airway Device – Services may use alternative advanced airway control devices (such as supraglottic
airways) as specified by the ambulance service’s medical director. After placement of an alternate advanced airway device,
place continuous end-tidal carbon dioxide (CO2) detection device on the tube.
Pulse Oximetry – A pulse oximeter should be used for any patient with suspected hypoxemia, in respiratory distress, or whenever
sedating medications are administered.
Revision Date: 10 April 2014
Revision Date: 10 April 2014
Ridgeview Ambulance Protocols
General Adult
Protocol 3020
DIABETIC HYPOGLYCEMIC PATIENT REFUSAL OF TRANSPORT
3020 - DIABETIC HYPOGLYCEMIC PATIENT REFUSAL OF TRANSPORT
Standing orders for all diabetic hypoglycemic patients refusing transport:
The following criteria must be documented on your Patient Care Report (PCR) in order to leave a patient
(without contacting medical control) experiencing a diabetic hypoglycemic emergency who refuses transport:
Identifiable reason to explain the hypoglycemia
Blood sugar greater than 100 post treatment
Awake, alert, & oriented, GCS 15 post treatment
Food available and/or eaten
Friend or family present to stay with the patient
Discussion with the patient to contact their primary care provider
Vital signs within normal limits
Not on oral agents besides metformin (Glucophage)
No suspected overdose of any diabetes medications
No recent fever, acute illness, other concerning symptoms such as chest pain, shortness of breath, etc.
If ALL of these conditions are met, it is not necessary to contact a medical control physician. If however, any
one of them is not met, contact medical control physician.
Paramedic also has discretion to contact medical control physician for any questions.
Revision Date: 15 November 2021
Revision Date: 15 November 2021
Ridgeview Ambulance Protocols
General Adult
Protocol 3030
FIREGROUND FIRE FIGHTER REHABILITATION
3030 - FIREGROUND FIRE FIGHTER REHABILITATION
Establish communication with Incident Command or rehab division officer.
Stage ambulance near rehab:
Consider egress and potential for additional incoming fire apparatus.
Perform focused assessment including complete set of vital signs and temperature (if applicable):
Consider 12-lead ECG.
Consider Blood Glucose check.
Consider transcutaneous CO measurement if available -
Administer high flow O2 immediately if concern for CO toxicity regardless of level or ability to measure.
Immediate transport for:
Symptoms of chest pain, severe SOB, altered mental status and syncope.
Heart rate greater than 220 (minus patient’s age), systolic blood pressure less than 100, respiratory rate greater
than 30, SpO2 less than 85%.
Treatment for immediate transport:
IV, O2, monitor, 12-lead ECG.
Consider hydroxocobalamin (Cyanokit) administration if available.
Begin active cooling/warming based on weather conditions.
Provide oral rehydration 8 - 12 oz/10 minutes.
Reassess the following after 10 minutes:
Vital signs.
Symptoms to assess for include:
Chest pain, dizziness, shortness of breath, weakness, nausea/vomiting, headache, cramps, change in behavior/speech,
unsteady gait.
If improving and asymptomatic, monitor until exit criteria met (see H):
Minimum 20 minute rest/rehydration time.
Offer transportation, if refused - document per service specific guidelines.
If worsening or symptomatic, transport:
IV, O2, monitor, 12-lead ECG, blood glucose check.
Consider hydroxocobalamin (Cyanokit) administration (per service specific guidelines).
“May return to work” criteria (must meet/document all below):
Offer of transport declined.
Presence of normal speech/mental status and a steady gait.
Normal vital signs:
Heart rate less than or equal to 110, respiratory rate less than or equal to 20, systolic blood pressure greater than 100,
diastolic blood pressure less than 100, SpO2 greater than 95%, skin temp normal or measured less than
101.5o F, CO less than 10 (if applicable).
Asymptomatic.
EMS provider discretion may override and recommend “no return to work” despite meeting criteria.
Revision Date: 13 October 2011
Revision Date: 13 October 2011
Ridgeview Ambulance Protocols
General Adult
Protocol 3040
INTRAVENOUS (IV) THERAPY
3040 - INTRAVENOUS (IV) THERAPY
Not every patient requires an IV. When indicated, intravenous fluid therapy should be administered in accordance with the following
guidelines:
For most patients requiring IV access, the paramedic has the option of either running fluids through the IV or capping
the catheter with a saline lock. However, as specified in these Medical Protocols, IV fluids must always be hung in
either situations:
When the administration of multiple IV medications is anticipated.
Whenever it is likely the patient will require fluid volume replacement.
There should be no delay at the scene for IV attempts on major trauma patients or patients in shock; these IVs should be started
during transport.
Intraosseous infusion (IO) is a procedure for use in patients who are in critical condition
when IV access is unobtainable.
Paramedics may access a Peripherally Inserted Central catheter (or PIC line) if the patient has one in place as an alternate IV
access point.
Paramedics may access a central line if the patient is in cardiac arrest. The cap on the central line must be cleansed with alcohol
and then 15-20 ml of fluid and blood must be aspirated from the central line before initiating IV fluids. If unable to aspirate, the
central line should not be used.
Acute (< 2 hrs duration) non-traumatic pain with 2 or more of the following:
Increased heart rate and/or blood pressure.
Nausea and/or vomiting.
Writhing.
Described as severe (or 8 - 10 / 10 on pain scale.)
Intubated patients with injury, painful condition or evidence of increasing discomfort (vital sign changes).
PROCEDURE
Assess the patient’s pain on a 0-10 scale or other acceptable method for patients with difficulty communicating.
Inform the patient that pain is an important diagnostic parameter and the goal of this protocol is to relieve suffering
and not to totally eliminate pain.
If the patient meets inclusion criteria, administer one of the following service dependent medications (consider lower
doses for elderly patients):
Not responding to initial 10 mg Morphine Sufate or 100 mcg fentanyl administration,
OR
If the patient has a Morphine Sulfate or fentanyl allergy,
BP < 90
0.1 mg/kg (not to exceed total dose of 10 mg) IV/IO/IM.
May repeat x 1 after 10 minutes for persistent pain.
Monitor the patient’s vital signs (including O2 saturation.) If respiratory depression or hypotension occurs after
administration of Morphine Sulfate -
For patients experiencing pain outside the above listed inclusion criteria consider:
Symptomatic relief of nausea/vomiting if needed
Advising them of the general concerns in the medical community about opioid use and that doctors are being very careful
about which patients receive these addictive medications
Inform them that “we carry this type of medication for severe trauma such as broken bones and for certain medical situations
that require immediate pain control such as heart attacks”
Acknowledge their pain and try to improve comfort
Advise them that a doctor will need to evaluate them prior to administering pain medication
Reassure the patient that the receiving facility will be notified of the need for prompt pain management assessment
Consult medical control if questions
AFTER OBTAINING VERBAL ORDERS
Consider initial or additional pain medication including benzodiazepines as appropriate:
Do not spend excessive time looking for the amputated part if the patient is unstable.
Amputated Part:
Wrap the amputated part in sterile gauze.
Moisten with saline.
Place in plastic bag.
Place on top of ice, if available, or cold packs (do not freeze).
Revision Date: 13 October 2011
Revision Date: 13 October 2011
Ridgeview Ambulance Protocols
Adult Trauma Protocols
Protocol 3120
BURNS
3120 - BURNS
Consider direct transport to a burn center for major burns (
2100 - Patient Disposition - Major Burns). Hospitals in the Twin Cities Metro area with a burn unit include:
Hennepin County Medical Center
Regions Medical Center
Major burn criteria includes:
Partial-thickness burns greater than 10% of total body surface area.
Partial-thickness or third degree burns that involve the face, hands, feet, genitalia, perineum, or major joint.
Third degree burns in any age group.
Lightning injury and other electrical burns.
Chemical burns.
Inhalation injury.
Burn in any patients with preexisting medical disorders that could complicate management, prolong recovery, or
affect mortality.
For any significant burn:
Begin oxygen therapy. Use positive pressure ventilatory assist as needed.
Obtain IV access.
If less than 20% of the body surface is burned:
Apply sterile dressings and saturate with cool water (leave Gel-pack(s) in place if applied by first responders).
Do not allow any burn patient to become chilled and begin shivering.
If more than 20% of the body surface is burned:
Remove any non-adherent burned clothing and cover the patient with a sterile sheet.
Consider NS bolus:
1,000 ml for patients 18 to 65.
500 ml for patients greater than 65 or history of CHF.
Do not cool down with water (exception: presence of smoldering clothes, articles or material adhering to skin that would
continue the burning process, e.g., hot tar, etc.).
Begin rapid transport.
Consider direct transport to a burn center for major burns.
Monitor the patient’s ECG after any electrical burn including a lightning strike.
Revision Date: 23 February 2023
Revision Date: 23 February 2023
Ridgeview Ambulance Protocols
Adult Trauma Protocols
Protocol 3130
CRUSH INJURIES
3130 - CRUSH INJURIES
Confirm prolonged entrapment (greater than one hour) of one or more full extremities by a crushing object
(e.g. vehicle, building rubble, hanging in harness, self).
If a distal extremity is accessible, assess sensation, motor function, skin color and distal pulses.
For entrapments with potential extended scene times (>30min), contact your service for notification/activation
of your service’s medical director(s).
Pre-Extrication, if possible:
Administer oxygen via mask if the situation allows.
Obtain venous access with two large bore IV/IOs when possible and hang two 1000 ml Normal Saline bags.
Administer up to two liters of NS bolus followed by 500 ml/hr.
If the patent begins to develop strong evidence of tension pneumothorax as indicated by the following clues, perform needle
thoracostomy at the fourth intercostal space, midaxillary line or second intercostal space, midclavicular line of the
affected side.
Absent or markedly diminished lung sounds
Hypotension
Tachycardia
Hypoxia or cyanosis
Increased respiratory distress or respiratory arrest
Lack of lung sliding sign on ultrasound
Transport quickly, minimize scene time
En route, obtain at least 2 points of IV/IO access and run normal saline wide open
IV/IO access should be started in route to the hospital. The only exception is when there is an unavoidable delay moving
the patient from the scene (e.g., trapped in auto, etc.) in which case IV/IO access should be started on scene.
Perform Bilateral needle decompression if obvious or suspected chest trauma
Secure airway with ETT, SGA, or OPA and ventilate with BVM
Establish IV or IO and initiate rapid administration of 500ml fluid bolus
Administer high quality chest compressions (only use mechanical CPR device during transport)
Re-assess per lines D and E (above) every 5 min
Transport to closest hospital is indicated for the following situations:
May consider immediate "load-and-go" for unsafe or hazardous scenes.
ROSC is achieved within 15 min
Penetrating trauma AND witnessed arrest AND within 10 min transport time
Pregnancy known > 24 weeks or fundus palpated above the umbilicus and within 10 min transport time
If transport criteria are not met after 15 min, contact medical control to consider termination of resuscitation
Revision Date: 20 July 2022
Revision Date: 20 July 2022
Ridgeview Ambulance Protocols
Adult Cardiac Protocols
Protocol 3210
CARDIAC ARREST (ASYSTOLE / PEA)
3210 - CARDIAC ARREST (ASYSTOLE / PEA)
Complete a rapid scene survey observing for any indications or evidence that resuscitation should not be
attempted (e.g., DNR orders or conditions incompatible with life.)
If cardiac arrest occurs in presence of the ambulance crew, assess the patient's cardiac rhythm and continue
with the appropriate protocol.
If patient is in cardiac arrest on arrival of the ambulance crew, institute or continue Basic Life Support (BLS):
Begin CPR using 30:2 Compression:Ventilation Ratio at a rate of 100-120 compressions/min.
Attach Impedance Threshold Device (ITD) to BVM
Apply to patient within 30 seconds. You must maintain a tight, continuous, 2- handed face mask seal
for the ITD to function properly
Reassess for presence of pulse/ reassess rhythm on cardiac monitor after every 5 cycles (2 minutes) of CPR
Limit interruptions in CPR to less than 10 seconds during pulse/ rhythm checks
Assess and confirm the patient's cardiac rhythm (check second lead to verify asystole,) immediately resume CPR.
Consider prompt administration of naloxone 4mg IN if not already given for any
suspicion of opioid overdose
Place an advanced airway – ETT (preferred initial) or i-Gel – while continuing compressions.
If ETT is placed, immediately confirm tube placement by exam and continuous EtCO2 waveform
Once advanced airway has been placed, ventilate at 10 breaths/min timed on compression upstroke.
DO NOT OVER VENTILATE
Monitor pulse oximetry and end-tidal CO2
Consider Reverting back to 30:2 if worsening SpO2
Obtain IV access while providing two minutes of continuous CPR.
Provide continuous CPR and reassess pulse and rhythm every two minutes.
Continue CPR and contact medical control physician for further orders.
AFTER OBTAINING VERBAL ORDERS
If the cause of PEA is hypovolemia, consider requesting additional fluid orders.
If there is no response, consider termination of resuscitative efforts.
Revision Date: 5 December 2024
Revision Date: 5 December 2024
Ridgeview Ambulance Protocols
Adult Cardiac Protocols
Protocol 3220
CARDIAC ARREST (V-FIB AND PULSELESS V-TACH)
3220 - CARDIAC ARREST (V-FIB AND PULSELESS V-TACH)
If cardiac arrest occurs in the presence of the ambulance crew, assess the patient's cardiac rhythm, and defibrillate
x1 if necessary
If patient is in cardiac arrest on arrival of the ambulance crew, institute or continue Basic Life Support (BLS):
Begin CPR using 30:2 Compression:Ventilation Ratio at a rate of 100-120 compressions/min.
Attach Impedance Threshold Device (ITD) to BVM
Apply to patient within 30 seconds. You must maintain a tight, continuous, 2- handed face mask seal for
the ITD to function properly
Reassess for presence of pulse/ reassess rhythm on cardiac monitor after every 5 cycles (2 minutes) of CPR
Limit interruptions in CPR to less than 10 seconds during pulse/ rhythm checks
Assess/ confirm pulseless Ventricular Fibrillation/ Ventricular Tachycardia then defibrillate x1 if necessary using the
following guidelines:
Continue CPR while the defibrillator is charging
Defibrillate at an initial dose of 200 joules
Immediately resume CPR
After patient receives defibrillation x1, continue CPR while preparing for likelihood of Refractory V-Fib/ Mobile
ECMO if patient meets criteria (refer to bullet ‘I’ below)
After patient receives defibrillation x2,
Tier 1 locations (ground) activate Refractory V-fib/ Mobile ECMO if patient meets criteria (refer to
bullet ‘I’ below)
Tier 2 locations (Air or ground transport delay) confirm that dispatch has activated Refractory V-fib/
Mobile ECMO if patient meets criteria (refer to bullet ‘I’ below and start helicopter transportation
(Life Link III)
Place an advanced airway – ETT (preferred initial) or i-Gel – while continuing compressions
If ETT is placed, immediately confirm tube placement by exam and continuous EtCO2 waveform
Once advanced airway has been placed, ventilate at 10 breaths/ min timed on compression upstroke
Continuous EtCO2 should be used to monitor airway status for any advanced airway
Obtain IV/IO access while providing continuous CPR. Administer the following medications:
Loading dose of 1 – 2 g IV/IO for possible Torsades de Pointes.
If patient has received at least 2 defibrillations, and the above interventions have been unsuccessful in achieving
ROSC, perform Dual Sequential Defibrillation OR Vector Change defibrillation, using the following guidelines:
If a second defibrillator (AED or Manual) is available
Place second set of pads in the unused position (ideally Anterior-Lateral)
If first pads are in the Anterior-Lateral position, ensure placement of Anterior-Posterior second set
does not take more than 10 sec during a pulse check pause.
When ready for next defibrillation attempt, continue compressions while charging both to 200J, when ready a
single provider should use one hand to shock with the AED first followed immediately by the manual device
with < 1 sec between shocks but not simultaneous.
If a second defibrillator (AED or Manual) is NOT available attempt Vector Change defibrillation as follows
Place a second set of pads in the unused location
if first pads are in Anterior-Lateral, ensure placement of Anterior-Posterior second set does not take more
than 10 sec during a pulse check pause
Deliver next defibrillation at 200 J via second pad position.
If there is no response to treatment, contact medical control for further orders and
consider termination of resuscitative efforts
Refractory V-Fib/ Mobile ECMO Activation: For patients who have received 1 defibrillation attempt (including from AED
prior to EMS arrival) without ROSC and who meet inclusion criteria below – contact W-MRCC as soon as possible (which may
be prior to EMS arrival) to activate mobile ECMO and begin transport to Fairview – Southdale (or other ECMO-capable site
as directed by ECMO team, family preference, and/or clinical history)
Inclusion criteria:
Age 18-75
V-Fib/V-Tach as initial rhythm (or AED shock)
Total CPR time expected to be < 60 minutes prior to ECMO flow
Chest size able to fit in LUCAS CPR device
Independently living
Arrest is presumed to be of cardiac etiology
Provide EARLY communication to W-MRCC with patient info (age, gender, pertinent clinical findings/ medical
history, ETA)
Use Verbiage “Red patient, Mobile ECMO activation” when hailing W-MRCC
Standby by tach channel assignment and communication with ECMO physician as needed.
Destination
Tier 1 locations: Ground transport destination (U of MN East Bank, Fairview Southdale or North Memorial)
will be determined by the ECMO team.
If Tier 1 location needing helicopter (ie major traffic
delay) coordinate LZ with Fire if needed
If inclusion criteria are not met, continue to provide cardiac arrest care per protocol above
If inclusion criteria are met, prioritize limiting scene time/ loading and transporting as quickly/ safely as
possible
Ensure First Responder help (two) and extra batteries for transport
Continue cardiac arrest management
Place patient on LUCAS CPR device
Place advanced airway (ETT preferred over i-Gel)
Change i-Gel to ETT if ineffective
ventilation
Obtain IV/IO access and administer epinephrine, at least first-dose of anti-arrhythmic (amiodarone or magnesium
sulfate) and 1 amp of sodium bicarbonate per protocol above
Provide EARLY communication to W-MRCC with patient info (age, gender, pertinent clinical findings/ medical
history, ETA)
Changes in condition (e.g. ROSC, PEA, asystole, etc.) should not change destination once activated
Patient/ family preference and clinical history (i.e. recent cardiac procedure) may supersede disposition to
alternate ECMO-capable facility (e.g. Abbott Northwestern)
Contact W-MRCC or call (612) 638-4901 if you wish to speak directly with a mobile ECMO
physician.
Revision Date: 1 March 2024
Revision Date: 1 March 2024
Ridgeview Ambulance Protocols
Adult Cardiac Protocols
Protocol 3230
ISCHEMIC CHEST PAIN
3230 - ISCHEMIC CHEST PAIN
Obtain 12-Lead ECG.
If STEMI is identified, apply defibrillation pads.
If the patient is allergic to Morphine Sulfate, may administer
fentanyl -
1 mcg/kg (up to 100 mcg per single dose) IV/IO.
If the patient meets the inclusion criteria as an ST Elevation Myocardial Infarction (STEMI) patient as defined in the
Metro Region STEMI Protocol the patient should be transported to a designated Level I Cardiac Center except as allowed
in the protocol. The receiving facility should be notified as soon as possible that the patient is a STEMI patient by
stating in your radio/phone report “STEMI ALERT.”
After Obtaining Verbal Orders
If the patient is a potential candidate for reperfusion therapy, consider diversion if the
difference in transport times to requested hospital versus closest hospital is greater than 30 minutes.
Revision Date: 23 February 2023
Revision Date: 23 February 2023
Ridgeview Ambulance Protocols
Adult Cardiac Protocols
Protocol 3240
PULMONARY EDEMA
3240 - PULMONARY EDEMA
Do not delay nitro to establish IV access.
Keep the patient’s head elevated at all times.
Begin oxygen therapy:
If the patient’s respiratory distress is severe -
Consider positive pressure ventilatory assistance if the patient is able to tolerate.
Consider ET intubation if when -
The patient's breathing is ineffective,
OR
The Glasgow Coma Score is less than 8.
Monitor the ECG closely for dysrhythmias secondary to hypoxia.
0.4 mg metered dose spray SL x 2 if the patient’s systolic BP is 140 or greater.
Two minutes after the initial nitro dose, repeat nitroglycerin 0.4 mg metered dose spray SL x 1 if
the patient still has signs of pulmonary edema AND the systolic BP remains 140 or greater.
Five minutes after the second dose, repeat nitroglycerin 0.4 mg metered dose spray SL x 1 if the
patient still has signs of pulmonary edema and the systolic BP is 140 or greater.
Administer 1mL (10mcg) of the epi every 2-5 minutes
Treat contributing causes.
Revision Date: 1 October 2022
Revision Date: 1 October 2022
Ridgeview Ambulance Protocols
Adult Cardiac Protocols
Protocol 3270
TACHYCARDIA
3270 - TACHYCARDIA
Tachycardia Flow Chart
Revision Date: 1 January 2020
Revision Date: 1 January 2020
Ridgeview Ambulance Protocols
Adult Respiratory Protocols
Protocol 3310
ASTHMA ATTACK
3310 - ASTHMA ATTACK
Asthma Flow Chart
Administer BiLevel CPAP to achieve 11 - 12 cm H2O IPAP (16 LPM) with EPAP set to lowest possible pressure. If
oxygenation status doesn't improve, increase EPAP to achieve desired SpO2.
Revision Date: 20 September 2020
Revision Date: 20 September 2020
Ridgeview Ambulance Protocols
Adult Respiratory Protocols
Protocol 3320
COPD (ACUTE EXACERBATION)
3320 - COPD (ACUTE EXACERBATION)
If the patient has a history of COPD and is symptomatic (presence of wheezing alone does not indicate COPD),
en route to hospital, the following may be administered:
Use a nasal cannula at 2 – 3 liters per minute initially. Oxygen may need to be increased if the patient’s
oxygenation status worsens.
When a patient is already on oxygen, EMS oxygen therapy flow rate should not start at a lower rate than
the patient’s current rate.
Oxygen flow should be titrated to a target SpO2 of 90%.
Consider CPAP if two or more of the following are present:
Retractions or accessory muscle use.
Pulmonary edema.
Respiratory rate greater than 25/min.
SpO2 less than 92%.
Administer BiLevel CPAP to achieve 11 - 12 cm H2O IPAP (16 LPM) with EPAP set to lowest possible
pressure. If oxygenation status doesn't improve, increase EPAP to achieve desired SpO2.
Assess the patient’s response. If the patient’s condition worsens, (e.g. the patient becomes hypotensive, decreased
SpO2) discontinue CPAP.
If CPAP is initiated, continue to treat with medications as normal.
AFTER OBTAINING VERBAL ORDERS
Treatment based on patient history and physical exam findings.
Revision Date: 20 September 2020
Revision Date: 20 September 2020
Ridgeview Ambulance Protocols
Adult Respiratory Protocols
Protocol 3330
KNOWN OUTBREAK OF TRANSMITTABLE RESPIRATORY ILLNESS (PATIENT IS BREATHING)
3330 - KNOWN OUTBREAK OF TRANSMITTABLE RESPIRATORY ILLNESS (PATIENT IS BREATHING)
To be used for patients with known or suspected transmittable respiratory illnesses in the presence of a known outbreak.
This would include patients who have a febrile illness with cough. Examples include -
Severe Acute Respiratory Syndrome (SARS),
Tuberculosis,
Epidemic influenza,
Others not listed here,
Protect yourself and crew with gowns, gloves and N95 mask/Powered Air Purifying Respirators (PAPR) and eye
protection.
Begin oxygen therapy by mask. If oxygen is not needed then place a surgical mask on the patient.
KNOWN OUTBREAK OF TRANSMITTABLE RESPIRATORY ILLNESS (PATIENT IS NOT BREATHING)
3340 - KNOWN OUTBREAK OF TRANSMITTABLE RESPIRATORY ILLNESS (PATIENT IS NOT BREATHING)
To be used for patients with known or suspected transmittable respiratory illnesses in the presence of a known outbreak.
This would include patients who have a febrile illness with cough. Examples include -
Severe Acute Respiratory Syndrome (SARS),
Tuberculosis,
Epidemic influenza,
Others not listed here,
Protect yourself and crew with gowns, gloves and N95 mask/Powered Air Purifying Respirators (PAPR) and eye
protection.
Insert oral airway and begin positive pressure ventilation.
Insert ET tube or other airway control device as authorized, as soon as possible. Use face shield (or Powered Air
Purifying Respirator if wearing one) for your eye protection during intubation.
For continued agitation, consider contacting a medical control physician for further orders.
AFTER OBTAINING VERBAL ORDERS
Consider additional droperidol (5-10 mg, max 20 mg) or midazolam hydrochloride (Versed)
(1-5 mg, up to max 10mg)
Co-administration of droperidol and benzodiazepines (i.e. Versed) may result in significant neurologic
and/or cardiovascular depression (especially hypotension). If co-administering these medications, it will
be necessary to closely monitor patient with end-tidal capnography and frequent blood pressure
monitoring.
COMBATIVE -
If the patient is combative with active physical violence to self or others evident, consider:
DO NOT attempt to place an IV in a severely combative patient.
If ketamine hydrochloride (Ketalar) is administered, rapidly move the patient to the ambulance and be
prepared to provide:
Respiratory support including suctioning, oxygen, and intubation.
Monitoring of the airway for laryngospasm (presents as stridor, abrupt cyanosis/hypoxia early in
sedation period). If laryngospasm occurs perform the following in sequence until the patient is
ventilating, then support as needed:
Once sedation has been administered, place the patient in a position where monitoring of condition and application
of monitoring equipment can be accomplished. Restraints may be used if necessary to ensure the continued safety of
the patient and providers.
Monitor the airway and be prepared to provide respiratory support including suctioning, oxygen, and intubation.
If LOC is not A or V on AVPU scale, utilize capnography and treat hypoventilation with ventilatory support
before SpO2 decreases
Consider IV access once sedation occurs (if no IV access previously established and Ketamine given IM) then
administer Normal Saline wide open up to 1 liter.
Consider Sodium Bicarbonate for extremely violent/combative patients that
required significant forceful restraint prior to sedation –
Consider transport directly to Hennepin County Medical Center for hyperbaric oxygen therapy.
Revision Date: 14 April 2016
Revision Date: 14 April 2016
Ridgeview Ambulance Protocols
Adult Medical Protocols
Protocol 3440
CEREBRAL VASCULAR ACCIDENT (CVA)
3440 - CEREBRAL VASCULAR ACCIDENT (CVA)
Assess ABCs and vital signs.
Provide oxygen via nasal cannula ONLY if SpO2 < 94% and establish IV access.
Check blood glucose level and treat if indicated.
Asses B.E.F.A.S.T. Stroke Scale
Balance: sudden loss of balance or coordination, SUSTAINED vertigo or vertigo with other focal
symptoms.
Eye: Bilateral visual field cut or double vision
Facial droop or weakness
Arm pronator drift or leg weakness
Speech difficulties, slurred speech, or aphasia (unable to repeat, name or follow simple
commands)
Thunderclap headache
Determine possible LVO (Large Vessel Occlusion)
Arm drift PLUS
Visual field cut OR
Aphasia OR
Neglect (forced lateral gaze or ignoring one side)
If B.E.F.A.S.T. is positive (abnormal findings)
If time of symptom onset is known to be within 24 hours, then:
Expedite transport - goal scene time < 15 min
Use "STROKE CODE" in radio report, and
Give time of symptom onset in clock time (e.g. 2:30 pm.)
If time of symptom onset is known to be greater than 24 hours, then:
Don’t use"STROKE CODE" in radio report, but do
State time of symptom onset (e.g. 2:30 pm) in your radio report
If time of symptom onset is unknown (e.g. “wake up” stroke or patient is unable to communicate), then:
Expedite transport - goal scene time < 15 min
Use "STROKE CODE" in radio report,
State "unknown symptom onset time,” and
Document last known well time on your PCR
Transport to facility of pt choice unless:
Possible LVO: Direct to Comprehensive (Abbott, HCMC, U of MN, North, Methodist, Regions, United) or
Primary -Thrombectomy capable (Southdale, Mercy) Stroke center.
Closer hospital if patient requested hospital (or LVO destination) adds more than 30 minutes or the
total transport time would be more than 45 min.
Closest hosptial if approaching 4 hrs since onset or last known well to stay within the 4.5 hr
cut off for possible thrombolytic therapy (including LVO patients).
Obtain ECG - 12 lead preferred.
Include the following information in your radio report
Time of onset (if known/certain) or last known well (clock time)
Description of focal deficit
ETA
Revision Date: 25 April 2024
Revision Date: 25 April 2024
Ridgeview Ambulance Protocols
Adult Medical Protocols
Protocol 3450
CHEMICAL EYE INJURIES
3450 - CHEMICAL EYE INJURIES
Attempt to remove the patient’s contact lenses, if present.
Immediately and continuously flush the affected eye(s).
Paramedics may insert Morgan lenses for irrigation if authorized.
Revision Date: 14 April 2016
Revision Date: 14 April 2016
Ridgeview Ambulance Protocols
Adult Medical Protocols
Protocol 3460
CHOLINERGIC EXPOSURE
3460 - CHOLINERGIC EXPOSURE
Hennepin County EMS Units are equipped with Duodote (Atropine 2.1mg/Pralidoxime 600mg) kits primarily for treatment of
responders. Chempack assets for mass casualty events can be activated via MRCC. Each Chempack treats up to 1000 patients
using Mark 1 kits (same as Duodote but separate injectors for atropine and pralidoxime), Atropens (atropine for pediatric
dosing), and diazepam auto- injectors for seizures.
Note – Chempack may contain Duodotes in the future and pediatric atro-pens may be eliminated.
Common cholinergic agents include: Carbamates (carbofuran (Fursban), etc.), Nerve gas agents (sarin, tabun, VX, etc.),
and Organophosphates (parathion, diazinon, malathion, chlorpyrifos (Dursban), etc.).
Recognize a toxidrome: Miosis (small pupils) present in ALL significant exposures in association with at least two of the
following:
Fasciculations
Respiratory distress
Increased secretions
Vomiting/diarrheas/incontinence
Seizure
Cardiovascular collapse
Request CHEMPACK activation from MRCC if mass casualty incident.
Wear appropriate personal protective equipment; DO NOT enter the hot
zone.
Assure appropriate patient decontamination measures if liquid or vapor exposures have occurred (in concert with fire
department/HazMat).
Assess the patient’s ABCs and begin oxygen therapy (when possible); intubate if needed (may have high airway
resistance).
Repeat as necessary to control bronchial secretions.
OR
CHEMPACK - Atropine IM 2 mg auto-injectors.
For patients with seizures, severe shortness of breath, and cardiovascular collapse administer:
2 Duodote auto-injector kits (600 mg Pralidoxime, 2.1 mg Atropine) or 2 Mark 1 kits (CHEMPACK).
Paramedics may administer one additional Duodote or Mark 1 kit after ten minutes if the patient continues to exhibit
severe symptoms and no IV access has been established.
Consider aggressive management of cardiac arrest if resources allow.
Revision Date: 13 October 2011
Revision Date: 13 October 2011
Ridgeview Ambulance Protocols
Adult Medical Protocols
Protocol 3470
DIABETIC EMERGENCIES
3470 - DIABETIC EMERGENCIES
Determine blood glucose level.
HYPERGLYCEMIA - If the patient’s blood glucose level is greater than 400 mg/dL and the patient is symptomatic:
Obtain IV access.
Give NS bolus -
500 ml for patients age 18 to 65.
250 ml for patients age who are greater than 65 or history of CHF.
Transport
HYPOGLYCEMIA - If blood glucose level is less than 60 mg/dL and the patient is symptomatic:
NOTE: For all IN doses that are ≤ 0.9 mL, add 0.1 mL to ensure full
dose of medication is given.
Due to the relatively short half-life of
naloxone hydrochloride (Narcan), patients that respond favorably to naloxone (Narcan) administration should
still be considered under the influence and transported on a peace/health officer hold (aka transport hold)
regardless of their mental status and/or refusal of care.
For all suspected tricyclic overdoses, monitor ECG.
Other treatments based on the patient history and physical exam findings.
Revision Date: 12 October 2017
Revision Date: 12 October 2017
Ridgeview Ambulance Protocols
Adult Medical Protocols
Protocol 3510
HYPOTHERMIA
3510 - HYPOTHERMIA
Standing orders for all hypothermic patients:
Remove wet garments.
Protect against further heat loss and wind chill (use blankets and insulating equipment).
Maintain the patient in a horizontal position.
Avoid rough movement and excess activity.
Monitor the patient’s cardiac rhythm.
Assess responsiveness, breathing and pulse.
Do a pulse check for 30 to 45 seconds (clinical signs of death may be misleading).
Pulse and breathing present:
Begin oxygen therapy.
Begin transport immediately.
Obtain IV access in route.
Monitor ECG.
Rewarming:
Mild hypothermia (temperature greater than or equal to 92o F or if
the patient is shivering) - Passive rewarming, active external rewarming.
Moderate hypothermia (temperature greater than or equal to 86o F
to less than 92o F, or if patient is shivering) - Passive rewarming, active external rewarming to truncal
areas only (neck, armpits, groin).
Severe hypothermia (temperature less than 86o F) - Transport for
active internal rewarming.
Pulse and breathing not present - Generally, CPR should not be initiated if the patient:
Is known to have been submerged (head under water) in cold water for more than 90 minutes.
Has obvious signs of death (e.g. decapitation, slippage of skin, animal predation).
Is frozen (e.g. ice formation in the airway).
Has a chest wall that is so stiff that compressions are impossible.
For pulseless patients with or without an organized ECG rhythm who do not meet criteria in part C and resuscitation
efforts are initiated:
Withhold medication treatments and further shocks and transport immediately.
Obtain IV/IO access.
Warm packs should not be used.
AFTER OBTAINING VERBAL ORDERS
Paramedics may consider cardiac arrest drugs and defibrillation but they are usually not effective until hypothermia is
corrected.
Revision Date: 8 October 2009
Revision Date: 8 October 2009
Ridgeview Ambulance Protocols
Adult Medical Protocols
Protocol 3520
LABOR AND DELIVERY
3520 - LABOR AND DELIVERY
If imminent delivery is not present, transport the patient in the position of comfort, usually on the patient’s left
side.
If in question of imminent delivery, observe briefly, then transport unless delivery is in progress.
Be prepared to stop the ambulance if delivery occurs en route.
If delivery is in progress:
Assist delivery using clean technique.
Suction the infant only if needed to clear obvious obstructions.
Protect from heat loss.
If no need for immediate resuscitation, wait 30-60 seconds then double clamp and cut the umbilical cord
approximately 8-10 inches from the infant.
Term infants (> 37weeks) who are crying (good respiratory effort) and have good muscle tone can be given to the
mother to nurse with continued warming efforts and re- assessment.
Age limits for pediatric patients must be flexible. For patients less than 13 years of age, pediatric orders should
always apply. Between the ages of 13 and 18 judgment should be used, although the pediatric orders will usually apply.
It is recognized that the exact age of a patient is not always known.
Parents should be allowed to stay with children during the evaluation and transport, if appropriate. The parent's
lap is usually the best place for the examination of a stable patient.
Paramedics may follow dosage and equipment recommendations listed on the Broselow Tape.
Bag Valve Mask (BVM) – Consider an oropharyngeal or nasopharyngeal airway of appropriate size on all unconscious
patients for initial airway maintenance.
Endotracheal intubation – After endotracheal intubation, tube position must be confirmed using at least two methods,
including continuous end-tidal carbon dioxide (CO2) detection and a second device or method to confirm tube
placement.
Alternate Advanced Airway Device – Services may use alternative advanced airway control devices (such as supraglottic
airways) as specified by the ambulance service’s medical director. After placement of an alternate advanced airway
device, place continuous end-tidal carbon dioxide (CO2) detection device on the tube.
Pulse Oximetry – A pulse oximeter should be used for any patient with suspected hypoxemia, in respiratory distress, or
whenever sedating medications are administered.
Revision Date: 10 April 2014
Revision Date: 10 April 2014
Ridgeview Ambulance Protocols
Pediatric General Protocols
Protocol 4020
INTRAVENOUS (IV) THERAPY
4020 - INTRAVENOUS (IV) THERAPY
Not every patient requires an IV. When indicated, intravenous fluid therapy should be administered in accordance with the
following guidelines:
For most patients requiring IV access, the paramedic has the option of either running fluids through the
IV or capping the catheter with a saline lock. However, as specified in these Medical Protocols, IV fluids
must always be hung in either situations:
When the administration of multiple IV medications is anticipated.
Whenever it is likely the patient will require fluid volume replacement.
There should be no delay at the scene for IV attempts on major trauma patients or patients in shock; these IVs should
be started during transport.
Intraosseous infusion (IO) is a procedure for use in patients who are in critical
condition when IV access is unobtainable.
Paramedics may access a Peripherally Inserted Central catheter (or PIC line) if the patient has one in place as an
alternate IV access point.
Paramedics may access a central line if the patient is in cardiac arrest. The cap on the central line must be cleansed with
alcohol and then 15-20 ml of fluid and blood must be aspirated from the central line before initiating IV fluids. If unable
to aspirate, the central line should not be used.
Revision Date: 9 October 2014
Revision Date: 9 October 2014
Ridgeview Ambulance Protocols
Pediatric General Protocols
Protocol 4030
PAIN MANAGEMENT
4030 - PAIN MANAGEMENT
To provide relief of pain when indicated.
Exclusion criteria:
Is hypotensive (i.e. clinical signs of poor perfusion, capillary refill greater than two seconds) or
per 9090 - Pediatric Reference Chart.
Except ketamine
Complains of abdominal pain
Has sustained a head injury
Pain determined to be cardiac in origin
Active labor
Headache
Non-traumatic Neck or Back Pain
Any chronic pain (e.g. head, neck or back pain, fibromyalgia, abdominal or pelvic pain.)
Dental pain.
Inclusion criteria:
Acute severe traumatic pain -
Neck or back pain from trauma and inability to ambulate from the incident.
Significant orthopedic injury. (Severe tenderness to palpation with swelling, bruising and/or deformity.)
Severe traumatic chest or abdominal pain with tenderness to palpation.
Inform the patient and/or guardians that pain is an important diagnostic parameter and the goal of this protocol is to
relieve suffering, not totally eliminate pain.
If the patient meets inclusion criteria, administer one of the following service dependent medications:
Not responding to initial dose of Morphine Sulfate or fentanyl,
OR
If the patient has a Morphine Sulfate or fentanyl allergy,
Hypotension
0.1 mg/kg (maximum dose 10 mg) IV/IO/IM.
May repeat x 1 after 10 minutes for persistent pain.
NOTE: Refer to pediatric reference (e.g., Broselow Tape) if assistance is needed with pediatric vital signs or
drug dosage calculations.
Monitor the patient’s vital signs (including O2 saturation.) If respiratory depression or hypotension
occurs after administration of Morphine Sulfate -
For patients experiencing pain outside the above listed inclusion criteria consider:
Symptomatic relief of nausea/vomiting if needed
Advising them of the general concerns in the medical community about opioid use and that doctors are being very
careful about which patients receive these addictive medications
Inform them that “we carry this type of medication for severe trauma such as broken bones and for certain medical
situations that require immediate pain control such as heart attacks”
Acknowledge their pain and try to improve comfort
Advise them that a doctor will need to evaluate them prior to administering pain medication
Reassure the patient that the receiving facility will be notified of the need for prompt pain management
assessment
Consult medical control if questions
AFTER OBTAINING VERBAL ORDERS
Consider initial or additional pain medication as appropriate.
Monitor for respiratory depression when administering narcotics and benzodiazepines together.
Revision Date: 30 January 2024
Revision Date: 30 January 2024
Ridgeview Ambulance Protocols
Pediatric Trauma Protocols
Protocol 4110
AMPUTATIONS
4110 - AMPUTATIONS
Patient:
Control hemorrhage and cover stump with sterile dressing saturated with saline.
Do not spend excessive time looking for the amputated part if the patient is unstable.
Amputated Part:
Wrap the amputated part in sterile gauze.
Moisten with saline.
Place in plastic bag.
Place on top of ice, if available, or cold packs (do not freeze).
Revision Date: 13 October 2011
Revision Date: 13 October 2011
Ridgeview Ambulance Protocols
Pediatric Trauma Protocols
Protocol 4120
BURNS
4120 - BURNS
Consider direct transport to a burn center for major burns (
2100 - Patient Disposition - Major Burns). Hospitals in the Twin Cities Metro area with a burn unit include:
Hennepin County Medical Center
Regions Medical Center
Major burn criteria includes:
Partial-thickness burns greater than 10% of total body surface area.
Partial-thickness or third degree burns that involve the face, hands, feet, genitalia, perineum, or major joint.
Third degree burns in any age group.
Lightning injury and other electrical burns.
Chemical burns.
Inhalation injury.
Burn in any patients with preexisting medical disorders that could complicate management, prolong recovery, or affect
mortality.
For any significant burn:
Begin oxygen therapy. Use positive pressure ventilatory assistance as needed.
Obtain IV access.
If less than 20% of the body surface is burned:
Apply sterile dressings and saturate with cool water (leave Gel-pack(s) in place if applied by first responders).
Do not allow any burn patient to become chilled and begin shivering.
If more than 20% of the body surface is burned:
Remove any non-adherent burned clothing and cover the patient with a sterile sheet.
Give 20 mL/kg NS bolus.
Do not cool down with water (exception: presence of smoldering clothes, articles or material adhering to skin that
would continue the burning process, e.g., hot tar, etc.).
Begin rapid transport and contact a medical control physician for further orders and destination decision.
Consider direct transport to a burn center for major burns.
If the patent begins to develop strong evidence of tension pneumothorax as indicated by the following clues, perform needle
thoracostomy at the fourth intercostal space, midaxillary line or second intercostal space, midclavicular line of the
affected side.
Absent or markedly diminished lung sounds
Hypotension
Tachycardia
Hypoxia or cyanosis
Increased respiratory distress or respiratory arrest
Lack of lung sliding sign on ultrasound
Transport quickly, minimize scene time
En route, obtain at least 2 points of IV/IO access and run normal saline wide open
IV/IO access should be started in route to the hospital. The only exception is when there is an unavoidable delay moving
the patient from the scene (e.g., trapped in auto, etc.) in which case IV/IO access should be started on scene.
Complete a rapid scene survey observing for any indications or any evidence that resuscitation should not be
attempted (e.g., DNR orders or conditions incompatible with life).
If cardiac arrest occurs in the presence of the ambulance crew, assess the patient’s cardiac rhythm and continue
with the appropriate protocol.
If the patient is in cardiac arrest on arrival of the ambulance crew:
Institute or continue BLS.
CPR: compressions 100/min, breaths 20 - 30/min.DO NOT OVER VENTILATE
Reassess the patient’s rhythm after every 5 cycles (2 minutes) of CPR. Limit interruptions in CPR during
pulse/rhythm checks to less than 10 seconds for airway insertion and/or administration of medications.
During CPR, administer epinephrine IV/IO, 0.01 mg/kg every 3-5 min. (1:10,000, 0.1 mL/kg)
Assess and confirm the patient’s cardiac rhythm, immediately resume CPR.
Review the most frequent causes for PEA, treat according to protocols if present:
Secure the patient’s airway during the pulse check. Continue CPR immediately then confirm tube placement by exam and
confirmation device.
Obtain IV access while providing two minutes of continuous CPR.
Provide continuous CPR and reassess, checking the patient’s pulse/rhythm every two minutes.
Contact medical control physician for further orders.
AFTER OBTAINING VERBAL ORDERS
If no response consider termination of resuscitative efforts.
Revision Date: 8 April 2021
Revision Date: 8 April 2021
Ridgeview Ambulance Protocols
Pediatric Cardiac Protocols
Protocol 4220
CARDIAC ARREST (V-FIB AND PULSELESS V-TACH)
4220 - CARDIAC ARREST (V-FIB AND PULSELESS V-TACH)
If cardiac arrest occurs in the presence of the ambulance crew -
Assess the patient’s rhythm
Defibrillate x 1 if necessary (energy rates as prescribed by current AHA ACLS guidelines; e.g., 2 J/kg.).
If the patient is in cardiac arrest on arrival of the ambulance crew, institute or continue BLS:
CPR: compressions 100/min, breaths 20 - 30/min.DO NOT OVER
VENTILATE.
Reassess the patient’s rhythm after every 5 cycles (2 minutes) of CPR.
Limit interruptions in CPR during pulse/rhythm checks to less than 10 seconds for airway insertion and/or
administration of medications.
Reassess the patient’s cardiac rhythm after 5 cycles (2 minutes) of CPR; if a shockable rhythm is present then
defibrillate x 1 using the following guidelines:
Continue CPR while the defibrillator charges.
Defibrillate x 1 (energy rates as prescribed by current AHA ACLS guidelines; e.g., 2 J/kg.).
Immediately resume CPR.
Secure the patient’s airway during the pulse check, then confirm tube placement by exam and confirmation
device.
Obtain IV access while providing two minutes of continuous CPR. Transport early if no readily accessible IV/IO
access.
NOTE: Refer to pediatric reference (e.g., Broselow Tape) if assistance is needed with drug dosage calculations
for pediatric patients.
Reassess the patient’s cardiac rhythm after 5 cycles (2 minutes) of CPR, if a shockable rhythm is present then
defibrillate x 1 using the following guidelines:
Continue CPR while the defibrillator charges.
Defibrillate x 1 (energy rates as prescribed by current AHA ACLS guidelines; e.g., 2 J/kg.).
Assess and support the patient’s ABCs, provide oxygen and ventilation, and attach the cardiac monitor/defibrillator.
PROBABLE SINUS TACHYCARDIA
Probable sinus tachycardia is defined as a QRS duration normal for the patient’s age (approximately less than or equal
to 0.08 sec). An infant’s heart rate is usually less than 220 bpm; a child’s heart rate is usually less than 180 bpm.
If hemodynamically unstable:
Continue to assess and support ABCs, monitor, and provide oxygen and ventilation as necessary.
Search for and treat underlying cause.
Consider Normal Saline bolus 20 mL/kg IV/IO.
PROBABLE VENTRICULAR TACHYCARDIA
Probable ventricular tachycardia is defined as a QRS duration wide for the patient’s age (approximately greater
than 0.08 sec). If hemodynamically unstable:
Perform synchronized cardioversion:
Energy rates as prescribed by current AHA ACLS guidelines:
0.5-1.0 J/kg; if not effective, increase to 2 J/kg
Use sedation if possible but do not delay cardioversion.
Probable supraventricular tachycardia is defined as a QRS duration normal for the patient’s age (approximately less than
or equal to than 0.08 sec). An infant’s heart rate is usually greater than or equal to 220 bmp; a child’s heart rate is
usually greater than or equal to 180 bpm. If hemodynamically unstable:
Consider vagal maneuvers (no delays).
If IV access is readily available give adenosine IV -
0.1 mg/kg IV (Maximum first dose 6 mg).
May double first dose and repeat once (Maximum second dose 12 mg).
Use rapid bolus technique.
If IV access is not readily available perform synchronized cardioversion:
Energy rates as prescribed by current AHA ACLS guidelines:
0.5-1.0 J/kg; if not effective, increase to 2 J/kg
Use sedation if possible but do not delay cardioversion.
25 mg/kg IV/IO over 3 to 5 minutes. Dilute (any dose) to 10 ml, total volume and given over 10 min.
MAXIMUM DOSE - 2 Gm
If hypotensive response to magnesium sulfate -
Administer 20 mL/kg normal saline bolus.
If the patient is unresponsive to other treatments and impending respiratory failure is evident consider advanced
airway.
Revision Date: 1 May 2019
Revision Date: 1 May 2019
Ridgeview Ambulance Protocols
Pediatric Respiratory Protocols
Protocol 4320
ASTHMA ATTACK (PATIENT IS NOT BREATHING)
4320 - ASTHMA ATTACK (PATIENT IS NOT BREATHING)
Insert an oral or nasal airway and begin positive pressure ventilation. Ventilate with a
short inspiration: long expiration ratio at a rate of 8 - 10/min.
Recommended dosage of 5 mg (5 ml) or as specified by service medical director.
If unable to administer epinephrine via neb, may administer epinephrine
0.01 mg/kg 1:1000 IM. Maximum dose 0.5 mg
Revision Date: 24 February 2022
Revision Date: 24 February 2022
Ridgeview Ambulance Protocols
Pediatric Respiratory Protocols
Protocol 4340
FOREIGN BODY AIRWAY OBSTRUCTION (FBAO)
4340 - FOREIGN BODY AIRWAY OBSTRUCTION (FBAO)
If the patient is making efforts to clear their airway without success, you may assist with careful back blows
(slaps) and chest thrusts for infants (less than one year old), and abdominal thrusts for children (greater than
or equal to one year old) per BCLS guidelines.
Synchronize with the patient's cough.
Avoid abdominal compressions in infants less than one year old.
If the patient has lost consciousness, attempt to open the airway (use moderate extension and jaw-lift) and
ventilate the patient with a bag-valve-mask (BVM). Reposition and attempt ventilation again if the initial attempt
was unsuccessful. If ventilations are unsuccessful, perform standard obstructed airway maneuvers for an infant or
child as appropriate.
Position an infant with the head dependent during back blows and chest compressions.
Consider direct laryngoscopy and foreign body removal with Magill forceps.
Attempt endotracheal intubation.
Transport early.
Revision Date: UNKNOWN
Revision Date: UNKNOWN
Ridgeview Ambulance Protocols
Pediatric Medical Protocols
Protocol 4410
ANAPHYLAXIS/ALLERGIC REACTION
4410 - ANAPHYLAXIS/ALLERGIC REACTION
For signs and symptoms consistent with anaphylaxis:
Consider additional personnel to adequately and safely restrain the patient.
If the patient is agitated and not amenable to reassurance, verbal de-escalation, or physical restraints, and
poses an immediate threat to himself/herself or others -
Hennepin County EMS Units are equipped with Duodote (Atropine 2.1mg/Pralidoxime 600mg) kits primarily for
treatment of responders. Chempack assets for mass casualty events can be activated via MRCC. Each Chempack treats up to 1000
patients using Mark 1 kits (same as Duodote but separate injectors for atropine and pralidoxime), Atropens
(atropine for pediatric dosing), and diazepam auto-injectors for seizures.
Note – Chempack may contain Duodotes in the future and pediatric atro-pens may be eliminated.
Common cholinergic agents include: Carbamates (carbofuran (Fursban), etc.), Nerve gas agents (sarin, tabun, VX,
etc.), and Organophosphates (parathion, diazinon, malathion, chlorpyrifos (Dursban), etc.).
Recognize a toxidrome: Miosis (small pupils) present in ALL significant exposures, in association with at least two
of the following:
Fasciculations
Respiratory distress
Increased secretions
Vomiting/diarrheas/incontinence
Seizure
Cardiovascular collapse
Request CHEMPACK activation from MRCC if mass casualty incident.
Wear appropriate personal protective equipment; DO NOT enter the hot
zone.
Assure appropriate patient decontamination measures if liquid or vapor exposures have occurred (in concert with fire
department/HazMat.)
Assess the patient’s ABCs and begin oxygen therapy if possible; intubate if needed (may have high airway
resistance.)
Treat seizure per protocol with midazolam (or CHEMPACK – Diazepam 10 mg auto injector IM only if > 25
kg.)
In cases of known organophosphate overdose/exposure or in a setting of multiple casualty incident (MCI) with patients
exhibiting this toxidrome:
Administer atropine sulfate IV
0.1 mg/kg IV/IO/IM (up to 2 - 5 mg/dose); repeat as necessary to control bronchial secretions
CHEMPACK – may contain auto injectors appropriate for:
Infant < 6 months = 0.5 mg infant (blue)
Todler < 2years = 1mg (red)
> 2 years old = 2 mg (standard Duodote or Mark 1 kit)
For patients with seizures, severe shortness of breath, and cardiovascular collapse administer Duodote auto-injector
if available (or Mark 1 kit from CHEMPACK):
2 - 10 years of age – 1 Duodote/Mark 1
> 10 years of age – 2 Duodote/Mark 1 kits per adult protocol
Paramedics may administer one additional Duodote (or Mark 1) kit after ten minutes if the patient continues to
exhibit severe symptoms and no IV access has been established. IV atropine is preferred in pediatric
patients.
Consider aggressive management of cardiac arrest if resources allow.
Revision Date: 13 October 2011
Revision Date: 13 October 2011
Ridgeview Ambulance Protocols
Pediatric Medical Protocols
Protocol 4440
DRUG INGESTION OR OVERDOSE
4440 - DRUG INGESTION OR OVERDOSE
For any patient with -
Respiratory rate less than eight,
OR
Has a history of opioid overdose,
OR
Has physical findings consistent with opioid overdose,
Due to the relatively short half-life of naloxone hydrochloride (Narcan), patients that respond favorably to
naloxone hydrochloride (Narcan) administration should still be considered under the influence and transported on a
peace/health officer hold (aka transport hold) regardless of their mental status and/or refusal of care.
For all suspected tricyclic overdoses, monitor ECG.
May give Glucagon 1 mg IM if IV access is difficult
or impossible to obtain.
A medical control physician must be contacted in any case where the patient experienced a
hypoglycemic event and the parent or guardian refused medical transportation.
Revision Date: 25 October 2022
Revision Date: 25 October 2022
Ridgeview Ambulance Protocols
Pediatric Medical Protocols
Protocol 4470
HYPOTHERMIA
4470 - HYPOTHERMIA
Standing orders for all hypothermic patients:
Remove wet garments.
Protect against further heat loss and wind chill (use blankets and insulating equipment.)
Maintain the patient in a horizontal position.
Avoid rough movement and excess activity.
Monitor the patient’s cardiac rhythm.
Assess responsiveness, breathing and pulse.
Do a pulse check for 30-45 seconds (clinical signs of death may be misleading.)
Pulse and breathing present:
Begin oxygen therapy.
Begin transport immediately.
Obtain IV access en route.
Monitor ECG.
Rewarming:
Mild hypothermia (temperature greater than or equal to 92o F or if
the patient is shivering) - Passive rewarming, active external rewarming.
Moderate hypothermia (temperature greater than or equal to 86o
F to less than 92o F, or if patient is shivering) - Passive rewarming, active external rewarming to truncal areas
only (neck, armpits, groin).
Severe hypothermia (temperature less than 86o F) - Transport for active
internal rewarming.
Pulse and breathing not present - Generally, CPR should not be initiated if the patient:
Is known to have been submerged (head under water) in cold water for more than 90 minutes,
Has obvious signs of death (e.g. decapitation, slippage of skin, animal predation),
Is frozen (e.g. ice formation in the airway) or,
Has a chest wall that is so stiff that compressions are impossible.
For pulseless patients with or without an organized ECG rhythm who do not meet criteria in part C and resuscitation
efforts are initiated:
Begin CPR.
For VF/Pulseless VT defibrillate once as prescribed by current AHA ACLS guidelines.
4220 - Cardiac Arrest (V_Fib and Pulseless V_Tach).
Withhold medication treatments and further shocks and transport immediately.
Obtain IV access and contact medical control physician en route.
Warm packs SHOULD NOT be used.
AFTER OBTAINING VERBAL ORDERS
Paramedics may consider cardiac arrest drugs and defibrillation but they are usually not effective until hypothermia is
corrected.
Revision Date: 8 October 2009
Revision Date: 8 October 2009
Ridgeview Ambulance Protocols
Pediatric Medical Protocols
Protocol 4480
NEWBORN EMERGENCIES
4480 - NEWBORN EMERGENCIES
In all situations, minimize the newborn’s heat loss:
Dry the newborn well.
Increase environmental temperature.
Suction the newborn only if needed to clear secretions or an obstruction:
During or after delivery, suction the mouth and oropharynx first, then the nose.
If meconium is present at birth, and the infant has poor muscle tone and inadequate respiratory
effort, keep warm and provide ventilatory assistance and oxygenation as needed, including intubation and suction if
the airway is obstructed.
During the first minute warm the infant, position airway, clear secretions if needed, and dry and stimulate.
Assess for apnea, gasping, or heart rate less then 100:
If apneic, gasping, or heart rate less than 100, initiate positive pressure ventilation, monitor SpO2,
and consider ECG monitoring.
If labored breathing or persistent cyanosis, reposition airway and administer oxygen (less then 30% FiO2).
Reassess heart rate:
If less than 100: correct ventilation of increase oxygen.
If less than 60: start chest compressions, increase oxygen to 100%, and intubate.
Continue to reassess heart rate.
If heart rate remains less then 60, administer epinephrine 1:10,000
(0.02 mg/kg) IV/IO.
Transport early. Attempt to maintain body temperature and assure optimal ventilation and oxygenation.
If patient is still seizing after two doses contact medical control.
Revision Date: 16 April 2016
Revision Date: 16 April 2016
Ridgeview Ambulance Protocols
Appendicies
Protocol 9020
TRAUMA TEAM ACTIVATION
9020 - TRAUMA TEAM ACTIVATION
General Principals of Activation
All TRAUMA TEAM MEMBERS in contact with the patient should wear personal protective equipment:
Gowns
Gloves
Masks to include eye shields
Only those designated should speak to the patient.
Appropriate victim exposure must be achieved. Everyone must be vigilant to keep doors closed in order to maintain
privacy.
Two large bore IV's (or an IO) will be placed on all adult trauma patients and one largest possible IV (or an IO) will
be initiated on all pediatric patients.
If gun shot or criminal injury noted through clothing, avoid cutting this area of clothing in order to preserve as
much of the evidence as possible. Save all clothing for proper collection in ED.
Notification
EMS identifies a patient meeting criteria for a TRAUMA TEAM ACTIVATION.
EMS calls the ED on PATIENT INFORMATION and relays the following information:
"RED PATIENT - TRAUMA TEAM ACTIVATION"
Provide a report with:
Rig Number
ETA
TTA CODE T# as described below-
Patient Name
DOB
Other Emergent Special Needs
M. Herold MD - November 2020
EMS relays to dispatch patient is a TRAUMA TEAM ACTIVATION, TTA CODE T#, as well as ETA to ED.
Upon arrival in ED:
Give report following "TTA TIMEOUT" procedure (Mechanism, Injuries, Symptoms with Vitals/GCS,
Treatment, Questions).
Transfer patient from EMS stretcher to ED bed.
Assist with patient care as directed.
Prepare ambulance and equipment for potential transfer to another facility.
Creation Date: 23 July 2018
Creation Date: 23 July 2018
Ridgeview Ambulance Protocols
Appendicies
Protocol 9021
MECHANICAL VENTILATOR MANAGEMENT - ADULTS
9021 - MECHANICAL VENTILATOR MANAGEMENT - ADULTS
Indications:
For patients with an advanced airway (ETT, SGA) secured in place with good waveform capnography
Only to be used during transport of the patient, including patients that are being mechanically
ventilated prior to arrival (i.e. interfacility transports)
Contraindications:
Lack of secure advanced airway with good waveform capnography
Patient with a known or suspected pneumothorax
Sustained ventilator alarms with an inability to correct
Patients weighing < 20 kg
Procedure:
For patients not previously mechanically ventilated - once patient is in the ambulance, they can be placed on the
ventilator. Start all patients on new adult setting.
For patients being mechanically ventilated upon arrival - EMS ventilator settings should be set to match existing
settings.
Settings can be adjusted as necessary to maintain goal oxygen saturation between 92-94% and ETCO2 between 35-45 mmHg. The
following are guidelines to stay within:
Tidal Volume – between 6-8 cc/kg
Follow the chart below for volume based on Ideal Body Weight.
Respiratory Rate – between 8-20 breaths/min
PEEP – 5-10 cmH2O
FiO2 – between 21-100%, titrated to maintain goal oxygen saturation 92-94%
Inspiratory Time – 1.0
Maintain ETCO2 between 35-45 mmHg
For ETCO2 < 35
Initial step: decrease respiratory rate to minimum of 8 breaths/ min
If issue persists: decrease tidal volume to minimum of 6 cc/kg
For a ETCO2 > 45
Initial step: increase respiratory rate to maximum of 20 breaths/ min
If issue persists: increase tidal volume to maximum of 8 cc/kg
Maintain oxygen saturation between 92-94%
Initial step: increase FiO2 in a step-wise fashion to 100%
If issue persists: increase PEEP to a maximum of 10 cmH2O
Ensure adequate sedation
Contact Medical Control Physician with any concerns, particularly:
If ventilator settings need to exceed above limits to maintain oxygen and ETCO2 goals
If patient is not otherwise tolerating ventilator settings
If patient’s height is not represented on Ideal Body Weight chart below
VENT Settings Chart
from "XYZ"
Creation Date: 1 October 2022
Creation Date: 1 October 2022
Ridgeview Ambulance Protocols
Appendicies
Protocol 9022
QUICK SET-UP GUIDE TO NIPPV (BPAP OR CPAP)
9022 - QUICK SET-UP GUIDE TO NIPPV (BPAP OR CPAP)
Press and hold “On/Standby” until lights turn on.
Turn selection wheel/dial on front lower-right face of machine
until “NEW PATIENT” is displayed at top of the machine. Press “Select” to the left of screen.
Turn dial until “ADULT” is displayed and press “Select”.
To silence alarm press “Silence Reset” on the right (and use repeated as needed as alarm comes back on after a time
lapse).
Selecting NPPV mode:
Press the grey button 3rd to the right from the bottom left, “Assist/Ctrl, SIMV/CPAP, NPPV” four times.
“NPPV” is flashing green and “SIMV/CPAP” is solid green
The only variable that is highlighted (with a default setting of “10”) is “Pres. Support.” All other variables will
have numbers that are dimmed.
Proceed to step 6 or 7 depending on desired positive airway pressure mode
BPAP (e.g., for usual initial orders are IPAP of 10 cm H20 and EPAP of 5 cm H20):
Dial “Pres. Support” down from “10” to “5.” Press the grey button beneath “Pres. Support” to confirm.
Note: Pressure Support = IPAP - EPAP.
“PEEP” now becomes highlighted. Turn selection wheel from “0” up to “5.” Press the grey button beneath “PEEP” to confirm.
Note: PEEP = EPAP
Change alarm settings to prevent continuous alarms:
Change “High Pres. Limit” to 100 using “Press, Change, Press” method.
Change “Low Pressure” to “—” using “Press, Change, Press” method.
Change “Low Min. Vol.” to “—” using “Press, Change, Press” method.
To change backup breath rate (default is 12 which is what is usually initially ordered):
Pressing the grey button beneath “Breath Rate”
Turn the dial so the desired rate is displayed
Press the grey button beneath “Breath Rate” again to confirm
To change FiO2:
Press the grey button beneath “O2%”
Turn the dial so the desired percentage is displayed
Press the grey button beneath “O2%” again to confirm
Change the display to read out the tidal volume
Press “Select” repeatedly until “Vte” appears on the display screen.
Tidal volume should remain consistent to assure NPPV is being properly delivered.
Tidal volume should be within 6-8mL/kg of ideal body weight.
Created: 8 February 2023
Created: 8 February 2023
Ridgeview Ambulance Protocols
Appendicies
Protocol 9023
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP)
9023 - CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP)
Continuous Positive Airway Pressure has been shown to rapidly improve vital signs, gas exchange, and the work of breathing,
decrease the sense of dyspnea, and decrease the need for endotracheal intubation in patients who suffer respiratory distress
from asthma, COPD, pulmonary edema, CHF, and pneumonia. In patients with CHF, CPAP improves hemodynamics by reducing preload
and afterload.
Any patient who is complaining of shortness of breath for reasons other than trauma and:
Is awake and able to follow commands.
Is over 12 years old and is able to fit the CPAP mask.
Has the ability to maintain an open airway.
A respiratory rate greater than 25 breaths per minute.
Has a systolic blood pressure above 100mmHg.
Uses accessory muscles during respirations.
Sign and Symptoms consistent with COPD, pulmonary edema/CHF.
Patient is in respiratory or cardiac arrest.
Patients suspected of having a pneumothorax (unequal breath sounds).
Patients at risk for vomiting.
Patient has a tracheostomy.
Use care if patient:
Has impaired mental status and is not able to cooperate with the procedure.
Has failed at past attempts at noninvasive ventilation.
Has active upper GI bleeding or history of recent gastric surgery.
Complains of nausea or vomiting.
Has inadequate respiratory effort.
Has excessive secretions.
Has a facial deformity that prevents the use of CPAP.
If utilizing CPAP with a portable O2 tank, pay particular attention to oxygen levels as small tanks can deplete
quickly. When in the ambulance it is preferable to utilize the on-board oxygen.
EXPLAIN THE PROCEDURE TO THE PATIENT.
Ensure adequate oxygen supply to ventilation device (100%).
Place the patient on continuous pulse Oximetry.
Place the delivery device over the mouth and nose.
Secure the mask with provided straps or other provided devices.
Use in CPAP MODE only at 11 - 12 cm H2O (15 LPM).
Check for air leaks.
Monitor and document the patient’s respiratory response to treatment.
Monitor vital signs at least every 5 minutes. CPAP can cause BP to drop.
Monitor LOC closely. Worsening LOC indicates impending respiratory arrest. Be prepared to discontinue CPAP and assist
ventilations.
Monitor and document the patient’s respiratory response to treatment.
Continue to coach patient to keep mask in place and readjust as needed.
If respiratory status deteriorates, remove device and assist ventilations as needed.
CPAP therapy needs to be continuous and should not be removed unless the patient can not tolerate the mask or experiences
continued or worsening respiratory failure.
Consider assisting ventilations manually if the patient is removed from CPAP therapy.
CPAP may be discontinued if patient improves dramatically but be prepared to reinstitute CPAP is needed.
CPAP should not be used in children under 12 years of age.
Bronchodilator nebulization may be placed in-line with CPAP circuit.
Do not remove CPAP until hospital therapy is ready to be placed on patient.
Most patients will improve in 5-10 minutes. If no improvement within this time, consider assisting ventilations
manually.
Watch patient for gastric distention. Be prepared for vomiting.
CPAP does not violate DNR Order.
Request ALS intercept if patient condition does not improve.
Created: 20 September 2020
Created: 20 September 2020
Ridgeview Ambulance Protocols
Appendicies
Protocol 9024
BALLOON PUMP PROTOCOL
9024 - BALLOON PUMP PROTOCOL
Indications:
For use in a cath lab emergency when requested by the cath lab staff
Contra-Indications:
Balloon pump not functioning
Balloon leak
Procedure:
When a cath lab emergency occurs, you will hear an overhead page in the hospital and the crew
should make their way to the cath lab expeditiously.
The cath lab team will be preparing to insert the balloon.
Balloon sizes are listed by height of patient. Smaller balloons can be used on larger
patients but not vice versa.
Remind the cath lab team that the balloon should remain in the sleeve as long as possible
otherwise it can unfurl and become difficult to insert. The team should also pull vacuum
on the balloon through a one-way valve and leave the valve on for insertion.
Turn on the balloon pump.
The on switch is on the left side of the balloon pump as you are looking at it from
the front.
Wait for the pump to say “System Test Okay”
Plug in the arterial line
For the orange fiber optic arterial line.
Match the red triangles when inserting.
You should see waveform spikes immediately.
For the fluid arterial line
Have the cath lab team assist in setting up the fluid arterial line.
Plug the fluid arterial line transducer into the grey cable with the oval receptacle.
Zero out the fluid arterial line by holding the “Zero Pressure” button for 2 seconds.
Plug helium line in through the safety ring
The safety disc should be tightly screwed in.
Assure that the helium tank is open.
Push start to start the balloon pump.
The balloon will start and stop as its initializing.
After approximately 34 seconds the pump should be functioning.
When you are able, attach the ECG.
Match green to green
All ECG leads can be placed in any order on the left side of the chest. Close
to the heart to assure a larger R wave.
If balloon pump is immobile:
Before 30 minutes of immobility:
Using a 3 way stop-cock and a large syringe pull vacuum on the helium line
and assure no blood (which would indicate a leak) appears in the line.
Then insert 40cc of air into the balloon and remove the air.
Repeat this process every 5 minutes.
If a balloon leak is suspected:
Confirm the presence of blood (rust or red or brown colored fluid) inside the helium
line. Wipe the outside of the line and confirm with a member of the cath lab team.
If a leak is confirmed stop the balloon pump immediately and inform the cath lab that
the balloon should be removed as soon as possible.
The helium line should be checked for leaks whenever the patient is moved.
Notes for the balloon pump
The mean pressure (MAP) should be 65 or greater. If it is not, inform the cath lab.
The pump will automatically adjust the timing. Do not manually adjust the augmentation or
timing.
The pump will automatically choose pressure or ECG for the trigger.
A rounded balloon pressure waveform could imply a kink in the balloon.
Created: 23 February 2023
Created: 23 February 2023
Ridgeview Ambulance Protocols
Appendicies
Protocol 9025
PARALYZATION FOR MECHANICALLY VENTILATED PATIENTS
9025 - PARALYZATION FOR MECHANICALLY VENTILATED PATIENTS
Purpose
To ensure patient and staff safety during transport of an adequately sedated adult patient, who is being mechanically
ventilated via endotracheal tube that has been previously confirmed to be in an appropriate position
This is NOT a mandatory action that needs to be taken on all intubated patients, rather, a tool available when needed
for appropriate indications
Indications
Possible scenarios when paralytics may be required include (but are not limited to):
Improving ventilator synchrony (e.g. patient is “bucking”/resisting ventilations, or patient is over-breathing
ventilator settings)
If there is a persistent risk of ETT dislodgement despite appropriately dosed sedation
This will be required even if patient is showing no signs of distress
Additional information
Patients experiencing their paralysis (awareness of paralysis) is a NEVER EVENT – it should never occur and must
be avoided in every instance. It is imperative that effective sedation is given during neuromuscular blockage to
avoid awareness of paralysis.
PATIENTS WEIGHT MUST BE ENTERED IN KILOGRAMS
Created: 1 July 2023
Created: 1 July 2023
Ridgeview Ambulance Protocols
Appendicies
Protocol 9026
AMBULANCE TRANSFERS REQUIRING A THIRD PERSON
9026 - AMBULANCE TRANSFERS REQUIRING A THIRD PERSON
Purpose: To assure adequate resources are available to provide safe care during interfacility transport.
Consideration/requirement criteria for needing addtional personnel:
Considerations:
Any patient requiring a 2:1 staff ratio to maintain stability.
Paramedic requests assistance based on patient's needs.
Hypotension requiring active titration of multiple vasopressors.
Suspected or imminent cardiovascular collapse.
Requirements:
Invasive pressure monitoring required:
Patient with an arterial line - requires a qualified RN or paramedic
Patient with a pulmonary artery catheter - requires a qualified RN
*If determined additional staff is needed for transport and unable to obtain, consider critical care transport or air
for transport.
Procedural Steps:
Unit staff advises dispatch of critically ill patient transfer and the potential "need for additional
staff" (meets one of the above consideration/requirement criteria).
- Dispatch gives estimated time of paramedic crew arrival to unit staff and deploys crew and paramedic
supervisor (if available) to patient location for team huddle.
Charge RN (or delegated to HUC) notifies the rest of the team member of huddle time (see checklist for 'who' should
huddle).
EMS staff and care team huddle and run checklist to discuss patient and need for additional staff for transport
based on the above consideration/requirement criteria
Unit staff secures and/or requests additional transport medications from pharmacy based on anticipated need
(minimum transport 45 minutes).
If it is determined that additional staff is required, the care team will quickly determine the most appropriate
team member to accompany the ambulance staff during transport.
- i.e., RN, RT, MD, Paramedic Supervisor, ED Tech, EMT etc.
When - to be used when a critically ill patient is being transported out of Ridgeview by the Ridgeview paramedic
team. (i.e. EDs, CICU, prep/recovery)
Who - bedside RN, paramedic team, charge RN, nursing supervisor, pharmacy (via phone at night), RT as needed
(i.e. patient vented or requires BiPAP), provider as appropriate
Where - team huddle at patient bedside
What - review below checklist items to determine what is needed for tranpsort
▢
Summary of patient/condition
▢
Vital signs and overall stability
▢
Current medication infusions, dose/rate
▢
Estimated transport time
▢
Estimate of infusion volume needed for transport
RN to obtain more medication for transport, as needed
Failure to stop bleeding with direct pressure or pressure dressing.
Injury does not allow for hemorrhage control with pressure.
Significant extremity hemorrhage in the face of any or all:
Need for airway management
Need for ventilator support
Circulatory shock
Need for other emergent interventions or assessment
Bleeding from multiple locations
Impaled foreign body with ongoing extremity bleeding.
Under fire or other dangerous situation for responding caregivers requiring immediate evacuation.
Total darkness or other adverse environmental factors.
Mass casualty, number of casualties exceeds ability to provide optimal care.
Tourniquet Application :
For severe bleeding associated with limb amputation or signs of shock with other exsanguinating hemorrhage,
skip to 4 (apply tourniquet).
Attempt to control bleeding with direct pressure or application of pressure dressing.
If profuse bleeding persists after 5 min or unable to maintain pressure due to other patient care needs, apply
a tourniquet (a commercial is preferred over an improvised tourniquet, but an improvised tourniquet is allowable
if a commercial tourniquet is not available)
Apply to appropriate extremity proximal to bleeding site over the humerus or femur only:
Tighten the self-adhering strap.
Tighten the windlass to loss of distal pulse.
Secure windlass in place.
Record time of application, preferably on extremity skin, or on tourniquet (if appropriate.)
Specify site and patient ID if multiple patients or sites.
Do not cover tourniquet unless risk of cold or environmental injury .
At 30 min of tourniquet time, reassess for removal: • If shock, clinically unstable, limited personnel/resources
or amputated extremity, DO NOT remove, otherwise, apply pressure dressing and loosen tourniquet (leave in place).
If re-bleeding occurs tighten to stop bleeding
Notify receiving healthcare personnel of tourniquet application time and location.
Revision Date: 13 October 2016
Revision Date: 13 October 2016
Ridgeview Ambulance Protocols
Appendicies
Protocol 9031
DIFFICULT INTUBATION - GUM-ELASTIC BOUGIE
9031 - DIFFICULT INTUBATION - GUM-ELASTIC BOUGIE
The ENDOTRACHEAL TUBE INTRODUCER (ETTI - aka bougie or Eschmann) is a semi-rigid device used to facilitate oral
tracheal intubation. It has a "hockey stick" end that eases insertion into the trachea even with sub-optimal
visualization. The endotracheal tube is then passed over the ETTI into the trachea.
Indications :
Incomplete visualization of the glotic opening during laryngoscopy for endotracheal intubation.
Contraindications :
Not to be used with endotracheal tubes less than 5.5 mm diameter.
Precautions :
Excessive force or passage beyond the carina may result in soft tissue damage or rupture of the bronchus.
Prepare for intubation per protocol, including preoxygenation, optimize positioning, suction & confirmation devices ready,
etc....
Lubricate ETTI with water-soluble jelly for dry oral pharynx as needed.
Perform laryngoscopy :
If no identifiable landmarks -
Suction / remove foreign matter if present.
Reposition laryngoscope.
Attempt BURP maneuver.
Consider immediate KING Airway placement versus reattemp after 30 to 60 seconds of BVM ventilation, then place KING
Airway.
If partial view of glotic opening -
Consider suction, reposition, BURP as above.
Use ETTI (see below.)
If complete visualization -
Pass ET tube on attempt per routine intubation protocol.
Use of ETTI for partial visualization of glotic opening -
Maintain glotic visualization with laryngoscope.
Pass ETTI through cords (if visable) or under epiglottis above arytenoids.
Note "clicks" as tip hits tracheal rings.
Advance to point of slight resistance when tip touches carina.
If no resistance is felt and depth is significantly past the black "lip line" marker -
OR
If no "clicks" felt -
The introducer is in the esophagus.
Have assistant slide the ET tube over the introducer until the far end of the introducer is through the ET tube.
Assistant then stabilizes the introducer and intubater takes the ET tube and continues passing it through the
cords. Maintain laryngoscopic visualization while advancing the ET tube to appropriate depth.
Rotate ET tube counter-clockwise 90o if slight resistance is noted.
Inflate cuff when intubator confirms complete insertion of ET tube.
Stablize ET tube while withdrawing introducer.
Remove laryngoscope.
Confirm tube placement with auscultation, ETCO2, SaO2, aspiration device and vapor in tube.
Secure ET tube in place.
Revision Date: 13 April 2017
Revision Date: 13 April 2017
Ridgeview Ambulance Protocols
Appendicies
Protocol 9032
ResQPOD
9032 - ResQPOD
The Res-Q-POD is a single use device that enhances circulation during
cardiopulmonary resuscitation by selectively impeding the inflow of respiratory gases during the recoil phase of
chest compressions.
Indications :
Cardiac Arrest
Contraindications :
Less than or appearing less than 12 years old and/or 100 pounds.
Any patient with a pulse and/or spontaneous respirations.
Select appropriate airway adjuct (BVM, King Airway, ETT.)
Use timing light with advanced airway (small red switch) during continuous CPR.
While performing CPR - place Res-Q-POD between the airway adjunct and ventilation delivery device.
Use C-collar for additional stabilization if intubated or when using King Airway.
If Res-Q-POD fills with blood, fluids or emesis - remove and shake fluid(s) out. Re-apply and continue circulation.
Remove Res-Q-POD if patient starts spontaneous respiration(s) or return of spontaneous circulation.
Revision Date: 13 April 2017
Revision Date: 13 April 2017
Ridgeview Ambulance Protocols
Appendicies
Protocol 9033
i-gel Airway
9033 - i-gel Airway
Indications :
Patient is unconscious and unable to protect own airway.
No apparent gag reflex.
Contraindications :
Patient with an intact gag reflex.
Ingestion of caustic substance(s).
Don protective eyewear, mask and gloves.
Ventilate patient with oral/nasal airways and BVM with 100% supplemental oxygen during preparation of i-gel.
Select appropriate size (Sized by ideal body weight):
#1 – for patients 2 kg - 5 kg (4 lbs - 11 lbs)
#1.5 – for patients 5 kg - 12 kg (11 lbs - 26 lbs)
#2 – for patients 10 kg - 25 kg (22 lbs - 55 lbs)
#2.5 - for patients 25 kg - 35 kg (55 lbs - 77 lbs)
#3 - for patients 30 kg - 60 kg (60 lbs - 132 lbs)
#4 – for patients 50 kg - 90 kg (110 lbs - 198 lbs)
#5 – for patients 90+ kg (198+ lbs.)
Open the i-gel package and on flat surface take out the protective cradle containing the device.
Remove the i-gel and transfer to the palm of the same hand that is holding the protective cradle, supporting the device
between the thumb and index finger.
Place a small bolus of a water based lubricant, such as K-Y Jelly, onto the middle of the smooth surface of the protective
cradle in preparation for lubrication.
Grasp the i-gel with the opposite (free) hand along the integral bite block and lubricate the back, sides and front of the
cuff with a thin layer of lubricant.
Grasp the lubricated i-gel firmly along the integral bite block. Position the device so that the i-gel cuff outlet is facing
towards the chin of the patient. The patient should be in the "sniffing" postion with head extended and neck flexed unless
you suspect c-spine injury, then place in a neutral in-line position. The chin should be gently pressed down before
proceeding.
Introduce the leading soft tip into the mouth of the patient in a direction towards the hard palate.
Glide the device downwards and backwards along the hard palate with a continuous but gentle push until a definitive
resistance is felt.
The tip of the airway should be located into the upper esophageal opening and the cuff should be located against the
laryngeal framework. The incisors should be resting on the integral bite-block.
Attach the manual resuscitator bag to the i-gel Airway device.
Confirm correct placement by listening for breath sounds, observing the chest rise and fall.
Secure the i-gel Airway device with tape or with the supplied head strap. Consider use of C-collar to restrict head
movement.
If using i-gel Airway device, consider decompressing the stomach by inserting a nasogastric tube through the gastric outlet
on the airway.
Removal of the airway is indicated -
IF the patient has a return of gag reflex AND ability to protect own airway,
OR
If ventilation is inadequate.
Don protective eyewear, mask and gloves.
Vomiting is likely, have suction ready with Yankauer tip.
If not contraindicated by suspected spinal injury, turn the patient to the side.
Carefully remove the i-gel Airway device staying alert for vomiting.
Oxygenate and ventilate as needed.
Sometimes a feel of "give-way" is felt before the end point resistance is met. This is due to the passage of the bowl of
the i-gel through the faucial pillars. It is important to continue to insert the device until a definitive resistance is
felt. Once definitive resistance is met and the teeth are located on the integral bite-block, do not repeatedly push
i-gel down or apply excessive force during insertion.
If there is early resistance during insertion -
A "jaw-thrust" (above) or "Insertion with Deep Rotation" (right) is
recommended.
It is not necessary to insert fingers or thumbs into the patients mouth during the process of inserting the device.
No more than three attempts in one patient should be attempted.
i-gel Airway Chart
from "IS6.3_igel_UK_issue_11_web.pdf"
Revision Date: 13 April 2017
Revision Date: 13 April 2017
Ridgeview Ambulance Protocols
Appendicies
Protocol 9034
EZ-IO
9034 - EZ-IO
Indications :
SIZE :
EZIO - AD for patients known or appearing to be 40kg or greater.
OR
EZIO - PD for patients 3kg to 39 kg.
Need for vascular access for volume replacement or medication administration in patients with poor venous access
or 2 failed IV attempts.
Decreased level of consciousness (GCS of 8 or below.)
Contraindications :
Patients known or appearing less than 3 kg.
Fracture(s) to long bones -
Leg Site(s) - Femur or tiba
Arm Site(s) - Humerus
Knee replacement (look for large anterior scar.)
Severe osteoporosis or tumor of leg / arm.
Infection at insertion site.
Inability to locate landmarks or excessive tissue at insertion site.
Considerations :
Use outside the above indications/contraindications may be authorized by online medical control.
EZ-IO driver.
EZ-IO needle set.
Arm Band.
Site prep.
Extension set.
10 ml syringe.
1 liter bag of normal saline.
External pressure device (or BP cuff.)
Tape/gauze.
2% Lidocaine (preservative free.)
Prepare the equipment, purge the tubing.
Prep the insertion site as per standard IV access technique.
Locate the patella, tibial tuberosity and flat surface of the tibia.
Insertion site is 1 finger width medial to the tuberosity.
Humeral head may be used as alternate site for patients with "leg" contraindications (above.)
Open the EZ-IO cartridge and attach needle set (confirm "snap".)
Remove needle cap with clockwise rotation.
Insert IO needle -
Stabliize extremity with one hand and position the driver over the site at a 90o angle to flat surface of
the bone.
Power the needle through the skin ONLY TO BONE SURFACE
Ensure the 5 mm mark (closest to the flange) on the catheter is visable.
If the mark is not visable, do not proceed, the needle set is not long enough.
Apply firm, steady pressure and power the needle into the bone until the flange touches the skin OR a
sudden lack of resistance is flet.
While supporting the needle set with one hand, pull straight back on the driver to detach from needle set.
Grasp the hub firmly with one hand and rotate the stylet counter clockwise until loose, pull it from the hub and place in
the styet cartridge.
Place the cartridge in biohazard container.
Confirm placement by :
Visable blood at tip of stylet,
Aspiration of marrow,
Free flow of fluid without evidence of leakage or extravasation.
Flush with 10ml of normal saline.
Secure catheter with tape/gauze.
Attach to 1 liter normal saline bag with external pressure device inflated to 300 mmHg.
Apply EZ-IO arm band.
Monitor for soft tissue swelling/leaks.
Locate the anatomical site
Place the patient's hand over the abdomen (elbow adducted and humerous internally rotated)
OR
With the elbow aganst the body, rotate the hand medially until the palm faces outward, thumb pointing down
Place you palm on the patient's shoulder anteriorly, the "ball" under your palm is the general targete area. You
should be able to feel this ball, even on obese pataients, by pushing deeply
Place the ulnar aspect of your hand vertically over the axilla and the ulnar aspect of your other hand along the
midline of the upper arm laterally
Place your thumbs together over the arm; nthis identifies the vertical line of insertion on the proximal
humerus
Palpate deeply up the humerus to the surgical neck. This may feel like gold ball on a tee - the spot where the
"ball" meets the "tee" is the surgical neck
The insertion site is 1 to 2 cm above the surgical neck, on the most prominent aspect of the greter
tubercle
Prepaire the skin / cleanse the area of insertion.
Load the appropriate needle into the driver - yellow needle
Firmly presse the needle set at a 45-degree angle to the anterior plane and posteromedial
As the needle reaches the bone, stop and be sure that the 5mm marking on the needle is visible; if it is,
continue to operate the driver
When a sudden decrease in resistance is felt and the flange ofhte needle rests against the skin, remove the driver and
the stylet from the catheter
Aspirate for blood/bone marrow(2nd confirmation of placement)
If the patient is responsive to pain - perform steps in "Pain" section
If no infiltration is seen, attach the IV line and infuse fluids and/or medications as normal
IV bag will need to be under pressure
Secure the needle
If drip rate is slow, flush with 10ml normal saline (5ml for EZIO-PD.)
Any medication that is administered by IV can also be administered by IO.
The device may be left in place for up to 24 hours.
Removal is accomplished by pulling while rotating the center hub counter clockwise.
Insertion of the EZIO-AD & EZIO-PD in conscious patients has been noted to cause mild to moderate discomfort (usually
no more painful than a large bore IV.) However, IO infusion for conscious patients has been noted to cause severe
discomfort -
Prior to IO syringe bolus (flush) or continuous infusion in alert patients, SLOWLY administer Lidocaine 2%
(Preservative Free) through the EZ-IO hub.
EZIO-AD : Slowly administer 20 mg to 40 mg Lidocaine 2% (Preservative Free.)
EZIO-PD : Slowly administer 0.5 mg/kg Lidocaine 2% (Preservative Free.)
Revision Date: 1 October 2022
Revision Date: 1 October 2022
Ridgeview Ambulance Protocols
Appendicies
Protocol 9035
CAPNOGRAPHY VIA NASAL CANNULA
9035 - CAPNOGRAPHY VIA NASAL CANNULA
To be used on select patients for monitoring of ventilatory status. This protocol does not apply to end-tidal
CO2 monitoring for patients that have undergone endotracheal intubation.
Indications
Undifferentiated shortness of breath
Patients receiving sedation
Patients with suspected opioid overdose, including those that have received naloxone
Contraindications
Cardiac arrest
In-line ETCO2 monitoring should be utilized with ETT or SGA use
Under no circumstances should the value of end-tidal CO2 interrupt routine ACLS cares (i.e. chest
compressions should not be discontinued early with changes in end-tidal CO2 values). If there is a
change appreciated in capnography, it is imperative to complete the round of compressions prior to pulse
check.
Revision Date: 27 April 2023
Revision Date: 27 April 2023
Ridgeview Ambulance Protocols
Appendicies
Protocol 9040
PAIN SCALES
9040 - PAIN SCALES
Wong-Baker Faces
Visual Analog Scale
FLACC Scale
Revision Date: 1 January 2019
Revision Date: 1 January 2019
Ridgeview Ambulance Protocols
Appendicies
Protocol 9045
INTERPRETER SERVICES
9045 - INTERPRETER SERVICES
Connect to Interpreter Now by Phone – Foreign Languages, CALL TOLL FREE 1-833-831-1598
Before the call:
Know the language that is needed. See next page for available languages.
Be prepared to brief the interpreter about the nature of the call before he or she speaks with the
limited English proficiency (LEP) patient.
For outbound calls, provide the operator with a dial out number. He or she will make a three way conference call.
How to call:
Dial 1-833-831-1598.
State the language that you need, your full name, your department name and the patient’s first and last name.
During the call:
Speak in short phrases or sentences.
Avoid slang, jargon, and technical terms.
Check for understanding from your LEP patient throughout the call.
When speaking to the interpreter, do not give and/or ask too much information at one time.
Ask questions in the first person.
Make sure to pause to allow the interpreter time to interpret and the LEP patient time to respond.
Ending the call:
Before ending the call, ensure that both the LEP patient and the interpreter know the session is about to end.
Revision Date: 24 February 2022
Revision Date: 24 February 2022
Ridgeview Ambulance Protocols
Appendicies
Protocol 9050
DO NOT RESUSCITATE (DNR) GUIDELINES
9050 - DO NOT RESUSCITATE (DNR) GUIDELINES
DO NOT RESUSCITATE (DNR) Flow Chart
Revision Date: 1 January 2019
Revision Date: 1 January 2019
Ridgeview Ambulance Protocols
Appendicies
Protocol 9060
EMSRB DNR FORM
9060 - EMSRB DNR FORM
Creation Date: UNKNOWN
Creation Date: UNKNOWN
Ridgeview Ambulance Protocols
Appendicies
Protocol 9070
MINNESOTA POLST FORM
9070 - MINNESOTA POLST FORM
Creation Date: UNKNOWN
Creation Date: UNKNOWN
Ridgeview Ambulance Protocols
Appendicies
Protocol 9080
HENNEPIN COUNTY PANFLU
9080 - HENNEPIN COUNTY PANFLU
These standing orders will be used to provide the best pre-hospital care to the greatest number of people during an extreme
situation. They will only be put into place when resources are defined by the system as “Level Red,” which means EMS services
are pending or not answering calls for which there is a significant risk of death for the patient. They do not supersede
other protocols. You will be notified when this status is in effect.
Our ethical commitments are:
Limitation of Individual Autonomy: The fair and just rationing of scarce resources requires public
health decisions based on objective factors, rather than on the choice of individual leaders, providers, or patients.
All individuals should receive the highest level of care given the resources available at the time.
Transparency: Governments and institutions have an ethical obligation to plan allocation through a
process that is transparent, open, and publicly debated. Governmental honesty about the need to ration medical care
justifies institutional and professional actions of withholding and withdrawing support from individual patients. These
restrictive policies must be understood and supported by medical providers and the public, ideally with reassurances
that institutions and providers will be acting in good faith and legally protected in their efforts.
Justice/Fairness: The proposed triage process relies on the principle of maximization of benefit to the
population served. The triage process treats patients equally based on objective, physiologic criteria, and when these
criteria do not clearly favor a particular patient, “first come, first serve” rules will apply.
Assurance: In order to ensure “procedural justice,” EMS triage processes will be regularly evaluated to
assure that the process has been followed fairly and consistently.
Documentation: MNTrac records will include policy notations including the times the “Level Red” was in
effect.
When an ambulance arrives on scene during “Level Red” status, instead of automatically offering transport to an emergency
department, as under normal practice, you will assess the patient’s objective condition and triage him/her into the following
categories:
Provide homecare information.
Refer to a clinic or other medical destination.
Refer to use of alternate transportation to a hospital, clinic or other medical destination.
Transport by (and at the descretion of) law enforcement.
Transport by ambulance to a hospital or other medical destination.
Standing Orders:
If the patient’s complaint or symptoms are not listed in this Appendix, Paramedic’s discretion is advised as long as the
decision is not in conflict with SOP.
When resources during a Pandemic are “Level Red,” automatically offer to transport patients with the following presentations:
1. Paramedic discretion - suspicion of critical injury/illness.
2. Altered vital signs (or age-specific abnormal vital signs,) including any one of these:
SBP < 90.
SpO2 < 92%.
RR > 30 (or respiratory distress.)
HR > 120, or delayed
capillary refill.
3. Breathinhg:
Respiratory distress.
Cyanosis or pallor/ashen skin.
4. Circulation/Shock:
Signs or symptoms of shock.
Severe/uncontrollable bleeding.
Large amounts of blood (or suspected
blood) in emesis or stool.
5. Neurologic:
Unconscious or altered level of consciousness.
New focal neurologic signs (CVA, etc.)
Status, multiple or new-onset seizure.
Severe headaches - especially sudden onset or accompanied with neck
pain/stiffness.
Head injuries with more than brief loss of consciousness or continued neck pain, dizziness, vision disturbances, ongoing
amnesia or headache, and/or nausea and vomiting.
6. Trauma:
Significant trauma with chest/spinal/abdominal/neurologic injury deemed unstable or potentially unstable.
Suspected fractures or dislocations that cannot be safely transported by private vehicle.
When resources during a Pandemic are “Level Red,” consider patients with the following presentations for:
transportation by ambulance - Note that many "transport by ambulance" patients will not require emergency transport to the hospital – in
which case, the crew may answer additional calls until the ambulance is full, or a critical patient is picked up,
depending on system call volumes.
transportation by alternate means - private vehicle or police to clinic or hospital. Except in very limited cases, the
patient should NOT self - transport to the hospital/clinic, but could be driven by someone else.
homecare - Give patient the homecare
form for their complaint and advise to contact personal medical provider if symptoms persist or worsen. The form will have
information pertaining to their complaint and list ways of caring for themselves, as well as what to look for that would
prompt self-transport to a clinic or hospital, or transport via ambulance to the hospital. Advise the patient that this
does not restrict them from seeking care at a clinic or hospital on their own, should they desire.
ABDOMINAL PAIN:
Pulsating mass.
Marked tenderness/guarding.
Pain radiating into
back and/or groin/inner thighs.
Recurrent severe vomiting not associated with diarrhea.
to
Recurrent severe vomiting associated with diarrhea - to emergency if
associated with signs/symptoms of dehydration, to urgent care or clinic if no dizziness nor vital sign
changes and normal exam.
Intermittent vomiting and diarrhea without blood or evidence of
dehydration.
ANAPHYLAXIS/STINGS:
Patients who have had epinephrine administered for symptoms.
Patients
experiencing airway, hypotension or respiratory symptoms, after an allergy exposure.
to
OR
Patients with itching after exposure - if rapid onset of symptoms, may require
EMS transport; if delayed > 1 hour, safe for private transport. All patients with history of anaphylaxis should be
seen in emergency room if possible. Others may be seen in clinic or urgent care. EMS may administer
diphenhydramine prior to clearing scene, up to 1mg/kg.
BACK PAIN:
Acute trauma with midline bony spinal tenderness.
New onset of extremity
weakness, sensory deficits, other neurological changes, incontinence of urine or bowel, urinary retention or
bloody urine.
Concern for abdominal aortic aneurysm.
Pain radiating into abdomen or groin/inner
thighs.
OR
Inability to ambulate/care for self.
Concern for kidney stone, bloddy urine.
BEHAVIORAL:
Uncontrolled agitation requiring sedation by EMS.
OR
OR
Suicidal ideation - must be left with a responsible party.
OR
Other emotionally disturbed patients may be transported at law enforcement's
discretion or by other means.
BLEEDING (LACERATIONS, ABRASIONS OR AVULSIONS):
Patient is on blood thinner(s) with significant ongoing bleeding or large hematoma.
to
Significant lacerations after bandaging - heavily contaminated, bite-related, likely
to involve foreign body, deep structure injury, sensory/motor deficit - to emergency room.
Lacerations
requiring simple repair - consider self- transport to physician's office or urgent care center (however, some
offices do not do procedures; patient will need to call ahead.)
Abraisions or avulsions not requireing suturing or repair, no significant
contamination
Minor lacerations that do not require sutures.
BURNS:
All chemical or electrical burns.
Suspected inhalant burn.
Significant
third degree burns.
Second degree burns to 5% or less BSA.
Second degree burns to face,
mouth.
Severe pain.
Second degree burns to hands or feet, or 1% to 5% BSA to other location(s) -
(size of patient's palmer surface.)
Second degree burns less than 1% BSA, non-critical location.
First degree
burns.
CARDIAC ARREST:
Witnessed down time of 10 minutes or less - follow usual resuscitation
protocol.
All others - report death to dispatch and return to service; do not wait for law
enforcement or medical examiner arrival.
CHEST PAIN:
Chest pain or other signs or symptoms suspicious for cardiac ischemia, pulmonary embolus,
or other life threat.
to
OR
Chest pain ongoing for over 12 hours and a normal ECG.
Pleuritic chest pain
without hypoxia.
Chest pain reproducible on physical exam to palpation is generally NOT concerning; unless ECG changes or known cardiac
disease,unlikely to require treatment for acute coronary syndrome.
DIABETIC:
OR
Any patient on oral diabetes medications with low blood glucose - if transported by
private vehicle must NOT drive self.
Critical high glucose or signs of Diabetic Ketoacidosis/
dehydration.
Patients with typical hypoglycemia and explanation for low sugar (did not eat, etc.) can
be left without medical control contact as long as family/friend is present and patient is eating.
ENVIRONMENTAL:
Heat-related illness with any alteration in mental status (confusion, decreased
LOC.)
Frozen extremity.
Hypothermia with AMS.
OR
Frostbite to face, hands, feet, other locations suspected deeper inury, blisters, or
frozen to touch.
Heat-related illness without alteration in mental status - initiate external cooling at
home under supervision of friends/family.
Minor frostbite with tissues now soft, pink, no blisters and NOT
involving digits.
ETOH/SUBSTANCE ABUSE:
Very decreased LOC or other confounding issues (head injury, suspicion of
aspiration.)
Otherwise may be transported at law enforcement's discretion.
Patient may be left with a responsible individual who can assist the patient.
Able to ambulate safely without assistance.
EYE PAIN:
Impaled objects or possible penetrating injury to eye, or globe rupture.
Chemical
esposures (alkaline) - after decontamination and initial rinsing.
OR
to
Eye pain and/or acute changes to vision should receive transport for urgent evaluation
to emergency department or other qualified clinic (e.g. eye clinic.)
Chemical exposures (non-alkaline) - consult
poison control for instructions; transport if symptoms/dangerous exposure.
Chemical exposures (non-alkaline) - consult poison control for instructions; if no
symptoms and limited toxicity likely, give instruction sheet.
FEVER:
Fever plus altered mental status including confusion.
Fever plus severe symptoms
by paramedic assessment.
Fever plau seizures, lethargy, stiff neck, rash or blistering.
OR
to
Fever estimated to be at or above 100.5o for three months or less - to
emergency room or clinic urgently.
History of fever greater then 3 months that does not reduce with anti-pyretics,
or fever lasting more then 5 days - emergency room, urgent care, or clinic.
HEADACHE:
With vision deficit, lethargy or other qualifies such as fever, etc.
New headaches for patient require assessment
Usual headaches for patient
may require treatment.
MUSCULOSKELETAL INJURIES (ISOLATED):
Loss of distal pulses.
Unable to effectively splint the affected body
part.
Neurological changes or deficits.
Open fractures.
Displaced fractures or pain requiring
injectable narcotics.
Suspected fractures that are stable and do not require injected analgesia may be
splinted appropriately and transported by private vehicle.
or
Neck pain and back pain after MVC that is delayed in onset and not associated with
midline tenderness or neurologic systems.
NOSE BLEED:
Signs of hypovolemia or dizziness upon standing.
Patient is on blood
thinners (Coumadin, lovenox, clopidogrel, etc.)
Continued high blood pressure (SBP > 200) in setting of
nosebleed.
Continued severe bleeding despite EMS efforts to control.
All others.
OB/PREGNANCY:
Imminent delivery.
Pain in abdomen or back.
Profuse vaginal
bleeding.
Third trimester (> 24 weeks) bleeding.
Pre/Eclampsia - syncope, seizure, altered mental
status, SBP equal to or greater then 140.
All others.
SWALLOWING PROBLEM:
Patient unable to manage own secretions due to pain or obstruction.
All others.
SYNCOPE:
History of coronary disease or heart failure.
Age of 55 or
over.
Pregnant.
Chest pain, headache or shortness of breath (or other symptoms concerning to
paramedics.)
to
OR
Likely dehydration with dizziness preceding the snycope.
Other underlying
medical conditions.
TOXICOLOGICAL:
or
to OR
Overdose or other toxic exposure - contact Poison Control and/or online medical
control.
If intentional - see section 4:Behavioral in this appendix.
VULNERABLE PERSON IN POTENTIAL DANGER:
EMS should assure that person will not be left in dangerous environment.
If safe disposition and transport can be arranged and the injuries do not otherwise require medical evaluation,
other transport may be appropriate.
Creation Date: 9 April 2009
Creation Date: 9 April 2009
Ridgeview Ambulance Protocols
Appendicies
Protocol 9090
PEDIATRIC REFERENCE CHART
9090 - PEDIATRIC REFERENCE CHART
Creation Date: UNKNOWN
Creation Date: UNKNOWN
Ridgeview Ambulance Protocols
Medication Reference 9903
ADENOSINE, IV
9903 - ADENOSINE, IV
Generic Name
adenosine IV
Trade Name
Adenocard IV
Classification
Antiarrhythmics
Indications
To convert acute PSVT to normal sinus rhythm. Includes PSVT associated with accessory bypass
tracts (Wolff-Parkinson-White syndrome.)
Contraindications
Patients with hypersensitivity to the drug. Those in second or third degree heart block, sick
sinus syndrome, or symptomatic bradycardia.
Adverse Effects
Chest pain, dizziness, dyspnea and/or shortness of breath, facial flushing, headache,
lightheadedness, blurred vision, nausea, metallic taste, and numbness. More serious symptoms are persistent arrythmias,
and bronchospasm.
Precautions
Could produce bronchoconstriction in patients with asthma. Patients who develop high level
heart block after a single dose should not receive additional doses. Use with caution in patients receiving digoxin and
verapamil in combination. Theraputic levels of theophylline and methylxanthines affect the response of adenosine.
Dipyridamole potentiates its effect.
Indicated for the relief of bronchospasm in patients two years of age and older with reversible
obstructive airway disease and acute attacks of bronchospasm.
Used with caution in patients with cardiovascular disorders, especially coronary
insufficiency, cardiac arrhythmias and hypertension. MAO inhibitors, tricyclic antidepressants, may potentiate action
on CV system. Propranolol and other beta blockers inhibit the effect of albuterol.
Ophthalmic procedures in which it can provide good local anesthesia (flushing eyes out after
chemical injury.)
Contraindications
Hypersensitivity to the drug.
Adverse Effects
Hypersensitivity reactions, conjunctival redness, transient eye pain, and lacrimation or increased
winking. A hyperallergic corneal reaction may occur which includes an acute diffuse epithelial keratitis.
Precautions
Should be used cautiously in patients with cardiac disease, or hyperthyroidism. Prolonged use may
produce permanent corneal opacification with loss of vision.
Concentration(s)
0.5% in 4 mL ampule
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9912
AMIODARONE HYDROCHLORIDE (CORDARONE)
9912 - AMIODARONE HYDROCHLORIDE (CORDARONE)
Generic Name
amiodarone hydrochloride
Trade Name
Cordarone
Classification
Antiarrhythmics
Indications
Used in a wide variety of atrial and ventricular tachyarrhythmias and for rate control of
rapid atrial arrhythmias in patients with impaired LV function when digoxin has proven ineffective.
Contraindications
Marked sinus bradycardia due to severe sinus node dysfunction, second-or third-degree AV
block, syncope caused by bradycardia (except when used with a pacemaker). Cardiogenic shock. Lactation.
Adverse Effects
Cough and progressive dyspnea. Worsening of arrhythmias, symptomatic bradycardia, sinus
arrest, SA node dysfunction, CHF edema, hypotension, cardiac conduction abnormalities, cardiac arrest, abnormal
involuntary movements, headache, nausea and vomitting, abdominal pain, flushing, and shock
Precautions
May produce vasodilation and hypotension. May have negative inotropic effects. May prolong
QT interval. Do not routinely use with other drugs that prolong QT interval. Use with caution if renal failure is
present.
Hypersensitivity to drug. Patients with active ulcer disease. Pediatric patients.
Adverse Effects
Bleeding gums, signs of GI bleeding, and petechiae. Aspirin will increase bleeding time.
Precautions
Use with caution in patients with GI lesions, impaired renal function, hypoprothrombinemia,
vitamin K deficiency, thrombocytopenia, or severe hepatic impairment.
Concentration(s)
81 mg per tablet
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9918
ATROPINE SULFATE IV
9918 - ATROPINE SULFATE IV
Generic Name
atropine sulfate IV
Trade Name
Atropine IV
Classification
Antiarrhythmic, anticholinergic, antidote.
Indications
Treatment of symptomatic sinus bradycardia or atrioventricular block at the nodal level. Usually
not effective when infranodal block suspected. Second drug for asystole or PEA.
Contraindications
Hypersensitivity to the drug, unstable cardiovascular status, myocardial ischemia, glaucoma, and
obstructive disease of the GI or GU tracts.
Adverse Effects
Postural hypotension, blurred vision, dryness of the mouth, GI reflux, nausea, vomiting,
paralytic ileus, tachyarrhythmias, and urinary retention.
Precautions
Use with caution in presence of myocardial ischemia and hypoxia. Avoid in hypothermic bradycardia.
Usually not effective in second degree block type II and third degree blocks with wide QRS complexes. Antacids decrease
absorption of med.
Concentration(s)
0.1 mg per 1 mL
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9921
IPRATROPIUM INHALATION (ATROVENT)
9921 - IPRATROPIUM INHALATION (ATROVENT)
Generic Name
ipratropium bromide
Trade Name
Atroven
Classification
Bronchodilators
Indications
Either alone or with other bronchodilators, especially beta andrenergics is used for treatment of
bronchospasm associated with chronic obstructive pulmonary disease, including asthma chronic bronchitis and emphysema.
Contraindications
Hypersensitivity to the drug, Atropine and its derivatives, and those with a history of
hypersensitivity to soy lecithin or related food products such as soybeans and peanuts.
Use cautiously in patients with angle-closure glaucoma, prostatic hyperplasia, and bladder-neck
obstruction. void leakage around the face mask, temporary blurring of vision or eye pain may occur.
Supplemental therapy to epinephrine in anaphylaxis and other uncomplicated allergic
reactions requiring prompt treatment.
Contraindications
Hypersensitivity to the drug, during acute asthmatic attacks, in newborns, and premature
neonates.
Adverse Effects
Palpitations, hypotension, tachycardia, confusion, insomnia, headache, vertigo, restlessness,
tremor, seizures, blurred vision, nausea and vomiting, and anaphylactic shock.
Precautions
Use with extreme caution in patients with prostatic hyperplasia, asthma or COPD,
increased intraocular pressure, hyperthyroidism, CV disease, or hypertension. Avoid SC or perivascular injection.
Potential CNS depression when used in the presence of sedating medications, alcohol, or other illicit substances.
Known or suspected hyperkalemia (e.g., renal failure), Hypocalcemia (e.g., after multiple blood
transfusion, and as an antidote for toxic effects (hypotension and arrhythmias) from calcium channel
blocker overdose or B-Adrenergic blocker overdose.
Contraindications
Hypersensitivity to the drug, digitalized patients, hypercalcemia, ventricular
fibrillation.
Adverse Effects
May cause bradycardia, cardiac arrest, metallic, calcium or chalky taste, prolonged state of
cardiac contraction, sense of oppression, or tingling sensation, especially with a too-rapid rate of administration.
(Overdose) nausea and vomiting, coma, and sudden death.
Precautions
Do not use routinely in cardiac arrest; do not mix with Sodium Bicarbonate. Three times more
potent then calcium gluconate. For IV use only.
Concentration(s)
100 mg per 1 mL
Revision Date: 1 January 2018
Revision Date: 1 January 2018
<
Ridgeview Ambulance Protocols
Medication Reference 9930
DEXTROSE IV
9930 - DEXTROSE IV
Generic Name
D-glucose or glucose
Trade Name
Dextrose IV
Classification
Nutritional (carbohydrate).
Indications
Diabetics who are unable to take oral fluids due to altered level of consciousness and low blood
glucose.
Contraindications
Delirium tremens with hydration, diabetic coma while blood sugar is excessive, hepatic coma
intracranial or intraspinal hemorrhage, glucose-galactose malabsorption syndrome.
Use with caution in patients with cardiac or pulmonary disease, hypertension, renal insufficiency,
urinary obstruction, or hypovolemia. Avoid extravasation which may cause tissue sloughing,
necrosis, and phlebitis.
Concentration(s)
500 mg per 1 mL (0.5 GRAMS per 1 mL)
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9932
DROPERIDOL (INAPSINE)
9932 - DROPERIDOL (INAPSINE)
Generic Name
Droperidol
Trade Name
Inapsine
Classification
Antipsychotic
Indications
Acute undifferentiated agitation
Contraindications
Known or suspected QT prolongation, including congenital long QT syndrome; not for use in
children < 2 years of age.
Precautions
Administer droperidol with extreme caution to patients who may be at risk for development of
prolonged QT syndrome (eg, congestive heart failure, bradycardia, use of a diuretic, cardiac
hypertrophy, hypokalemia,hypomagnesemia, or administration of other drugs known to increase
the QT interval). Other risk factors may include age greater than 65 years, alcohol abuse,
and use of agents such as benzodiazepines, volatile anesthetics, and IV opiates. Initiate
droperidol at a low dose and adjust upward, with caution, as neededto achieve the
desired effect.
Concentration(s)
2.5 mg/mL; consult specific product labeling.
Revision Date: 1 May 2023
Revision Date: 1 May 2023
Ridgeview Ambulance Protocols
Medication Reference 9933
EPINEPHRINE
9933 - EPINEPHRINE
Generic Name
epinephrine hydrochloride
Trade Name
Adrenalin
Classification
Cardiac stimulant, bronchodilator, antiallergic, and vasopressoR.
Indications
Cardiac arrest: VF, pulseless VT, asystole, pulseless electrical activity. Anaphylaxis, severe
allergic reactions, and profound bradycardia or hypotension.
Contraindications
Patients with angle-closure glaucoma, shock (other than anaphylactic shock), organic brain damage,
cardiac dilation, coronary insufficiency, cerebral arteriosclerosis or labor and delivery. Do not use to treat overdose
of adrenergic blocking agents.
Adverse Effects
Nervousness, tremor, headache, agitation, dizziness, weakness, cerebral hemorrhage, palpitations,
hypertension, tachycardia, anginal pain, nausea and vomiting, and dyspnea.
Precautions
High doses do not improve survival or neurologic outcome and may contribute to postresuscitation
myocardial dysfunction. Raising blood pressure and increasing heart rate may cause myocardial
ischemia, angina and increased myocardial oxygen demand. Higher doses maybe required to treat
poison/drug-induced shock. Do not use concurrently with Brevibloc. The effects of the drug maybe
potentiated by tricyclic antidepressants.
Concentration(s)
1 mg per 1 mL for 1:1000 (30 mL vial)||||| -
||||| 0.1 mg per 1 mL for 1:10,000 (pre-filled syringe)
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9934
EPINEPHRINE - PUSH-DOSE
9934 - EPINEPHRINE - PUSH-DOSE
Indications:
Anaphylaxis, refractory to IM epi
Sepsis, refractory to IV fluids
Bradycardia (Adult), not responding to atropine or pacing
Remove 1mL of normal saline from a 10mL flush, then draw up 1mL of
epinephrine (1:10,000). The result should be a 10mL syringe with 100mcg
of 1:10,000 Epi.
Alternatively you can draw 9mL of normal saline and 1mL of
epinephrine (1:10,000) into a 10mL syringe.
Vigorously roll the syringe to ensure it is well mixed.
Label the syringe.
Administration
Adult
Administer 1-2mL (10-20 mcg) of the epi every 2-5 minutes.
Titrate to systolic blood pressure > 90 mmHg
Pediatric
Administer 0.1ml/kg (1mcg/kg) (Maximum single dose 1 ml) of epi every 2-5 minutes
Titrate to systolic blood pressure > 70 mmHg
Revision Date: 25 April 2024
Revision Date: 25 April 2024
Ridgeview Ambulance Protocols
Medication Reference 9936
FENTANYL
9936 - FENTANYL
Generic Name
fentanyl
Trade Name
Duragesic, Subsys, Abstral
Classification
Opioid Analgesic
Indications
Control of pain associated with musculoskeletal pain.
Contraindications
Hypersensitivity to fentanyl or other fentanyl analogues. May cause muscle rigidity (including
muscles of respiration) if given in high dose or too rapidly.
May cause muscle rigidity (including muscles of respiration) if given in high dose or too
rapidly.
Concentration(s)
50 mcg per 1 mL
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9939
GLUCAGON
9939 - GLUCAGON
Generic Name
glucagon
Trade Name
GlucaGen
Classification
Antihypoglycemic, antidote, and diagnostic agent.
Indications
Treatment of severe hypoglycemia, helpful in reversing adverse beta-blockade of beta-
adrenergic blocking agents and calcium channel blockers, diagnostic aid in radiologic exam of abdomen.
Contraindications
Known hypersensitivity to drug, and in patients with pheochromocytoma or with insulinoma
(tumor of pancreas).
Adverse Effects
Hyperglycemia (excessive dosage), nausea and vomiting hypersensitivity reactions (anaphylaxis,
dyspnea, hypotension, rash), increased blood pressure, and pulse; this maybe greater in patients taking beta-
blockers.
Precautions
Give with caution to patients that have low levels of releasable glucose (e.g., adrenal
insufficiency, chronic hypoglycemia, and prolonged fasting). Potentiates oral anticoagulants. Depletes glycogen
stores especially in children and adolescents.
Concentration(s)
1 mg per 1 mL
Revision Date: 1 January 2019
Revision Date: 1 January 2019
Ridgeview Ambulance Protocols
Medication Reference 9945
KETAMINE HYDROCHLORIDE (KETALAR)
9945 - KETAMINE HYDROCHLORIDE (KETALAR)
Generic Name
ketamine hydrochloride
Trade Name
Ketalar
Classification
Non-barbiturate anesthetic.
Indications
Severely agitated patient that poses an immediate threat to himself/herself or others and
usual chemical or physical restraints may not be appropriate or safely used.
Contraindications
Ketamine is contraindicated in patients with any condition in which a significant elevation
of blood pressure would be hazardous such as: severe cardiovascular disease, heart failure, severe or poorly
controlled hypertension,recent myocardial infarction, history of stroke, cerebral trauma, intracerebral mass or
hemorrhage. Also contraindicated for hypersensivity to the drug.
Adverse Effects
Psychological manifestations varying in severity between pleasant dream-like states, vivid
imagery, hallucinations, nightmares or illusions and delirium. Other adverse effects
include: Diplopia, nystagmus, blood pressure and pulse rate elevations, and local pain and
exanthema at the injection site
Precautions
Barbiturates and Ketamine, being chemically incompatible because of precipitate formation,
should not be injected from the same syringe. Use with caution in the chronic alcoholic and the acutely
alcohol-intoxicated patient. The intravenous dose should be administered over a period of 60 seconds. More rapid
administration may result in respiratory depression or apnea and enhanced pressor response. Resuscitative
equipment should be ready for use.
Concentration(s)
100 mg per 1 mL
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9948
LIDOCAINE HYDROCHLORIDE, IV
9948 - LIDOCAINE HYDROCHLORIDE, IV
Generic Name
lidocaine hydrochloride IV
Trade Name
Xylocaine IV
Classification
Antiarrhythmic
Indications
Cardiac arrest from VF/VT (class II B) Stable VT, wide-complex tachycardias of uncertain type,
wide-complex PSVT (class IIB).
Contraindications
Hypersensivity to the drug. Stokes-Adams syndrome, Wolff-Parkinson-White syndrome, severe
degrees of SA, AV, or intraventricular block (when no pacemaker is present.)
Adverse Effects
Anaphylaxis, bradycardia, hypotension, cardiovascular collapse, seizures, malignant hyperthermia,
respiratory depression, tremors, lightheadedness, confusion, tinnitus, blurred or double vision, and
vomiting
Precautions
Prophylactic use in AMI patients is not recommended. Discontinue infusion immediately if
signs of toxicity develop. Elderly clients who have hepatic or renal disease or who weigh less then 45.5 kg should
be watched closely for adverse side effects. Do not add lidocaine to blood transfusion assembly. Potentiates
amiodarone, beta-adrenergic blockers (Inderal) and Tagamet. Toxicity can occur due to reduced metabolism of
lidocaine.
Concentration(s)
20 mg per 1 mL
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9951
MAGNESIUM SULFATE HEPTAHYDRATE
9951 - MAGNESIUM SULFATE HEPTAHYDRATE
Generic Name
Magnesium Sulfate heptahydrate
Trade Name
Magnesium Sulfate
Classification
Antiarrhythmic, electrolyte replenisher, and anticonvulsant.
Indications
Refractory VF (after lidocaine), torsades de pointes with a pulse, life threatening ventricular
arrhythmias due to digitalis toxicity, adjunctive to alleviate bronchospasm in acute asthma, control of seizures in
pregnancy, and control of hypertension in acute nephritis in children.
Contraindications
In the presence of heart block or myocardial damage, hypersensitivity to drug, and within 2 hours
preceding delivery of PIH patient.
Adverse Effects
CNS depression, hypotension, circulatory collapse, depression of myocardium. Sweating, hypothermia,
muscle paralysis, respiratory paralysis, suppression of knee jerk reflex, and changes in ECG,
(increased PR interval,increased QRS complex, and prolonged QT interval).
Precautions
Morphine and Valium potentiate respiratory depression when given to patient receiving MgSO4.
Calcium gluconate should always be available to treat possible respiratory depression due to MgSO4. Toxic level is >10
mg/dL.
To produce sedation, relieve anxiety, and impair memory of procedural events. Used with or without
narcotic for conscious sedation before short procedures. Also as a component in the induction of anesthesia before
administration of other anesthetic agents, and for patients in status seizures.
Contraindications
Hypersensitivity to the drug, and acute narrow-angle glaucoma. Not recommended in pregnancy,
childbirth, breast-feeding, shock, coma, acute alcohol intoxication with depression of vital signs.
Adverse Effects
Serious cardiorespiratory events (airway obstruction, apnea, hypotension, oxygen desaturation,
respiratory and or cardiac arrest), paradoxical behavior or excitement. Other common side effects are coughing,
headache, hiccups, nausea and vomiting, and nystagmus (especially in children).
Precautions
Use cautiously in patients with uncompensated acute illness and in elderly or debilitated patients.
Administer slowly over at least 2 minutes. Use with caution in neonates. Versed does not protect against the intracranial
pressure or against the pulse and blood pressure rise associated with intubation. Erythromycin may alter the
metabolism of Versed. Oral contraceptives prolong the half-life. Sedative effects may be antagonized by
theophylline.
Concentration(s)
5 mg per 1 mL
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9957
MORPHINE SULFATE, IV
9957 - MORPHINE SULFATE, IV
Generic Name
Morphine Sulfate
Trade Name
Morphine Sulfate (names may vary if preservative free)
Classification
Narcotic analgesic, adjunct, pulmonary edema.
Indications
Analgesic of choice in pain associated with myocardial infarction that is unresponsive to
nitrates. Treatment of acute pulmonary edema associated with left ventricular failure, if blood pressure is
adequate. Used for sedation, to decrease anxiety and facilitate induction of anesthesia.
Contraindications
Hypersensitivity to opiates, acute bronchial asthma, heart failure secondary to lung disease,
upper airway obstruction, acute alcoholism, convulsive states, and paralytic ileus.
Adverse Effects
Seizures (with large doses), hypotension, bradycardia, cardiac arrest, or may see tachycardia, and
hypertension. Nausea and vomiting, ileus, urine retention, respiratory depression and arrest, hypothermia, and increased
intracranial pressure may also been seen.
Precautions
Causes hypotension in volume-depleted patients. Administer slowly and titrate to effect. May
cause apnea in asthmatic patients. May also cause increase ventricular response rate in presence of
supraventricular tachycardias. Use with caution in the elderly, head injuries with increased
intracranial pressure, COPD, severe hepatic or renal disease.
Concentration(s)
10 mg per 1 mL
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9960
NALOXONE HYDROCHLORIDE (NARCAN) IV
9960 - NALOXONE HYDROCHLORIDE (NARCAN) IV
Generic Name
naloxone hydrochloride
Trade Name
Narcan
Classification
Narcotic (opioid) antagonist, Antidote.
Indications
Indicated for complete or partial reversal of known or suspected narcotic-induced respiratory
depression and overdose. Antidote for natural and synthetic narcotics. Also indicated for the
diagnosis of suspected opioid tolerance.
Contraindications
Hypersensitivity to the drug. The naloxone challenge test should not be performed in patients
showing S/S of withdrawal or whose urine contains opioids.
Adverse Effects
May see VF, tachycardia, hypertension, nausea, vomiting, and diaphoresis, in higher doses.
Tremors and withdrawal symptoms in narcotic-dependent patients.
Precautions
May precipitate acute withdrawal symptoms in narcotic addicts. Effects of drug may not outlast
effects of narcotics. Use with caution in patients with cardiac disease or those receiving cardiotoxic drugs. It is
ineffective against respiratory depression caused by barbiturates, anesthetics, other nonnarcotic agents, or
pathologic conditions.
Initial antianginal for suspected ischemic pain. Drug of choice in unstable anginaor CHF
associated with acute myocardial infarction, and suspected pulmonary edema when systolic blood pressure is greater
than 140.
Contraindications
Hypersensitivity to nitrates, head trauma with increased intracranial pressure, hypotensive
patients,severe bradycardia or tachycardia, RV infarction, Viagra within 24 hours, and severe
anemia.
Adverse Effects
Headache, transient episodes of light-headedness related to blood pressure changes, hypotension,
syncope, crescendo angina, rebound hypertension, and anaphylactoid reactions. Abdominal pain and vomiting may also be
seen.
Precautions
Do not shake aerosol spray container because this affects metered dose. Patient should sit
or lie down when taking this drug. Concomitant use of nitrates and alcohol may cause hypotension. Marked symptomatic
orthostatic hypotension may occur when calcium channel blockers and oral controlled-release nitroglycerin are used in
combination.
Concentration(s)
0.4 mg per spray
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9969
ORAL GLUCOSE
9969 - ORAL GLUCOSE
Generic Name
oral glucose
Trade Name
Glutose, Glucose Gel, Insta-Glucose, GlucoBurst
Classification
Antihypoglycemic
Indications
Hypoglycemia in a known diabetic with confusion or an altered level of consciousness.
Contraindications
Unconscious, unable to swallow, hypersensitivity to drug.
Adverse Effects
If ingested may cause irritation of the gastrointestinal tract, nausea, vomiting, and/or allergic
reaction.
Precautions
Reassess mental status to determine if drug has had an effect.
Maintenance of an adequate airway and respiratory support is critical. Eyes should remain closed
during paralysis to protect against damage to the corner (ulceration from drying). Accidental
administration may be fatal. Confirm proper selection of intended product and ensure that the
intended dose is clearly labeled and communicated, when applicable.
Concentration(s)
10 mg/mL in 10 mL vials; consult specific product labeling.
Revision Date: 1 July 2023
Revision Date: 1 July 2023
Ridgeview Ambulance Protocols
Medication Reference 9972
SODIUM BICARBONATE
9972 - SODIUM BICARBONATE
Generic Name
Sodium Bicarbonate
Trade Name
Sodium Bicarbonate
Classification
Electrolyte replenisher, alkalizing agent.
Indications
Metabolic acidosis caused by circulatory insufficiency resulting from shock or severe dehydration,
severe renal disease, cardiac arrest, primary lactic acidosis, tricyclic overdoses, and hyperkalemia.
Contraindications
Patients with metabolic or respiratory alkalosis, patients losing chlorides by vomiting or GI
suction, patients receiving diuretics known to produce hypochloremic alkalosis, and patients with hypocalcemia in which
alkalosis may produce tetany, hypertension, seizures, or heart failure.
Adverse Effects
Gastric distention, belching, flatulence, hypokalemia, metabolic alkalosis, hypernatremia,
hyperosmolarity, hyperirritability or tetany. Extravasation of IV Sodium Bicarbonate may cause
chemical cellulitis with tissue necrosis.
Precautions
Not recommended for routine use in cardiac arrest patients. Sodium Bicarbonate inactivates
norepinephrine, and dopamine, and forms a precipitate with calcium. Use with caution in the elderly with renal or
cardiovascular insufficiency with or without CHF.
Used for prevention and reversal of bronchospasm in patients with bronchial asthma and reversible
bronchospasm associated with bronchitis and emphysema.
Contraindications
Patients with hypersensitivity to drug or sympathomimetic amines, cardiac arrhythmias with
tachycardia or digitalis toxicity, uncontrolled hypertension, and any preexisting maternal medical conditions
adversely affected by beta-mimetic drugs.
Adverse Effects
Paradoxical bronchospasm with prolonged usage, nervousness, tremor, drowsiness, headache,
weakness, palpitations, tachycardia, heartburn, nausea, vomiting, and hypokalemia (with high doses).
Precautions
Use cautiously in patients with CV disorders, hyperthyroidism, diabetes, or seizure disorders.
Drug is not recommended for children under 12 years of age because of insufficient clinical data.
Protect ampule from light. Do not use if discolored. Significant changes in systolic and diastolic
blood pressure may occur in some patients.
Concentration(s)
1 mg per 1 mL
Revision Date: 1 January 2018
Revision Date: 1 January 2018
Ridgeview Ambulance Protocols
Medication Reference 9978
TRANEXAMIC ACID (TXA)
9978 - TRANEXAMIC ACID (TXA)
Background
Plasmin breaks down clots by degrading fibrin (fibrinolysis). Tranexamic Acid (TXA) is an amino acid that blocks plasminogen
from being converted to plasmin, thus tipping the balance from fibrinolysis toward clot formation.
Uncontrolled junctional (Groin or other non-compressible) bleeding
Adult 1 g IV/IO slow push
Peds 15 mg/kg IV/IO slow push
Apply direct pressure with gauze soaked with 1g TXA Topical
Severe uncontrolled epistaxis
Fold a 4x4 in half twice to form a 2x2
Saturate with TXA 500 mg
Gently insert into the affect side(s)
Place nose clamp for continued pressure
Severe Varicose vein bleeding
Consider If unable to control with direct pressure or patient is on anticoagulation
Form a ball shape with 4x4 gauze
Saturate with TXA 500 mg
Apply topically with ace wrap pressure
Post tonsillectomy oral hemorrhage – severe/persistent
Administer TXA via nebulizer 500mg (5ml)
In ALL CASES communicate TXA administration, DOSE and ROUTE to the receiving facility
Revision Date: 1 March 2025
Revision Date: 1 March 2025
Ridgeview Ambulance Protocols
Medication Reference 9981
ONDANSETRON (ZOFRAN)
9981 - ONDANSETRON (ZOFRAN)
Generic Name
ondansetron
Trade Name
Zofran
Classification
Antiemetic
Indications
Severe Nausea and vomiting.
Contraindications
Known hypersensitivity to any component of preparation, long QTc, or evidence of serotonin
syndrome on physical exam. Discuss with medical control before giving to a patient known
to be pregnant.
Adverse Effects
The most common reported adverse affects are headache, diarrhea, blurred vision, constipation,
fever and fatigue.
Precautions
Very rarely and predominantly with intravenous ondansetron, transient ECG changes including
QT interval prolongation have been reported.
For patients with an advanced airway (ETT, SGA) secured in place with good waveform capnography
Only to be used during transport of the patient, including patients that are being mechanically
ventilated prior to arrival (i.e. interfacility transports)
Contraindications:
Lack of secure advanced airway with good waveform capnography
Patient with a known or suspected pneumothorax
Sustained ventilator alarms with an inability to correct
Patients weighing < 20 kg
Procedure:
For patients not previously mechanically ventilated - once patient is in the ambulance, they can be placed on the
ventilator. Start all patients on new adult setting.
For patients being mechanically ventilated upon arrival - EMS ventilator settings should be set to match existing
settings.
Settings can be adjusted as necessary to maintain goal oxygen saturation between 92-94% and ETCO2 between 35-45 mmHg. The
following are guidelines to stay within:
Tidal Volume – between 6-8 cc/kg
Follow the chart below for volume based on Ideal Body Weight.
Respiratory Rate – between 8-20 breaths/min
PEEP – 5-10 cmH2O
FiO2 – between 21-100%, titrated to maintain goal oxygen saturation 92-94%
Inspiratory Time – 1.0
Maintain ETCO2 between 35-45 mmHg
For ETCO2 < 35
Initial step: decrease respiratory rate to minimum of 8 breaths/ min
If issue persists: decrease tidal volume to minimum of 6 cc/kg
For a ETCO2 > 45
Initial step: increase respiratory rate to maximum of 20 breaths/ min
If issue persists: increase tidal volume to maximum of 8 cc/kg
Maintain oxygen saturation between 92-94%
Initial step: increase FiO2 in a step-wise fashion to 100%
If issue persists: increase PEEP to a maximum of 10 cmH2O
Ensure adequate sedation
Contact Medical Control Physician with any concerns, particularly:
If ventilator settings need to exceed above limits to maintain oxygen and ETCO2 goals
If patient is not otherwise tolerating ventilator settings
If patient’s height is not represented on Ideal Body Weight chart below
VENT Settings Chart
from "XYZ"
Creation Date: 15 October 2023
Creation Date: 15 October 2023
Ridgeview Ambulance Protocols
Critical Care Protocols
Protocol CC0003
QUICK SET-UP GUIDE TO NIPPV (BPAP OR CPAP)
CC0003 - QUICK SET-UP GUIDE TO NIPPV (BPAP OR CPAP)
Press and hold “On/Standby” until lights turn on.
Turn selection wheel/dial on front lower-right face of machine
until “NEW PATIENT” is displayed at top of the machine. Press “Select” to the left of screen.
Turn dial until “ADULT” is displayed and press “Select”.
To silence alarm press “Silence Reset” on the right (and use repeated as needed as alarm comes back on after a time
lapse).
Selecting NPPV mode:
Press the grey button 3rd to the right from the bottom left, “Assist/Ctrl, SIMV/CPAP, NPPV” four times.
“NPPV” is flashing green and “SIMV/CPAP” is solid green
The only variable that is highlighted (with a default setting of “10”) is “Pres. Support.” All other variables will
have numbers that are dimmed.
Proceed to step 6 or 7 depending on desired positive airway pressure mode
BPAP (e.g., for usual initial orders are IPAP of 10 cm H20 and EPAP of 5 cm H20):
Dial “Pres. Support” down from “10” to “5.” Press the grey button beneath “Pres. Support” to confirm.
Note: Pressure Support = IPAP - EPAP.
“PEEP” now becomes highlighted. Turn selection wheel from “0” up to “5.” Press the grey button beneath “PEEP” to confirm.
Note: PEEP = EPAP
Change alarm settings to prevent continuous alarms:
Change “High Pres. Limit” to 100 using “Press, Change, Press” method.
Change “Low Pressure” to “—” using “Press, Change, Press” method.
Change “Low Min. Vol.” to “—” using “Press, Change, Press” method.
To change backup breath rate (default is 12 which is what is usually initially ordered):
Pressing the grey button beneath “Breath Rate”
Turn the dial so the desired rate is displayed
Press the grey button beneath “Breath Rate” again to confirm
To change FiO2:
Press the grey button beneath “O2%”
Turn the dial so the desired percentage is displayed
Press the grey button beneath “O2%” again to confirm
Change the display to read out the tidal volume
Press “Select” repeatedly until “Vte” appears on the display screen.
Tidal volume should remain consistent to assure NPPV is being properly delivered.
Tidal volume should be within 6-8mL/kg of ideal body weight.
Creation Date: 15 October 2023
Creation Date: 15 October 2023
Ridgeview Ambulance Protocols
Critical Care Protocols
Protocol CC0004
BALLOON PUMP PROTOCOL
CC0004 - BALLOON PUMP PROTOCOL
Indications:
For use in a cath lab emergency when requested by the cath lab staff
Contra-Indications:
Balloon pump not functioning
Balloon leak
Procedure:
When a cath lab emergency occurs, you will hear an overhead page in the hospital and the crew
should make their way to the cath lab expeditiously.
The cath lab team will be preparing to insert the balloon.
Balloon sizes are listed by height of patient. Smaller balloons can be used on larger
patients but not vice versa.
Remind the cath lab team that the balloon should remain in the sleeve as long as possible
otherwise it can unfurl and become difficult to insert. The team should also pull vacuum
on the balloon through a one-way valve and leave the valve on for insertion.
Turn on the balloon pump.
The on switch is on the left side of the balloon pump as you are looking at it from
the front.
Wait for the pump to say “System Test Okay”
Plug in the arterial line
For the orange fiber optic arterial line.
Match the red triangles when inserting.
You should see waveform spikes immediately.
For the fluid arterial line
Have the cath lab team assist in setting up the fluid arterial line.
Plug the fluid arterial line transducer into the grey cable with the oval receptacle.
Zero out the fluid arterial line by holding the “Zero Pressure” button for 2 seconds.
Plug helium line in through the safety ring
The safety disc should be tightly screwed in.
Assure that the helium tank is open.
Push start to start the balloon pump.
The balloon will start and stop as its initializing.
After approximately 34 seconds the pump should be functioning.
When you are able, attach the ECG.
Match green to green
All ECG leads can be placed in any order on the left side of the chest. Close
to the heart to assure a larger R wave.
If balloon pump is immobile:
Before 30 minutes of immobility:
Using a 3 way stop-cock and a large syringe pull vacuum on the helium line
and assure no blood (which would indicate a leak) appears in the line.
Then insert 40cc of air into the balloon and remove the air.
Repeat this process every 5 minutes.
If a balloon leak is suspected:
Confirm the presence of blood (rust or red or brown colored fluid) inside the helium
line. Wipe the outside of the line and confirm with a member of the cath lab team.
If a leak is confirmed stop the balloon pump immediately and inform the cath lab that
the balloon should be removed as soon as possible.
The helium line should be checked for leaks whenever the patient is moved.
Notes for the balloon pump
The mean pressure (MAP) should be 65 or greater. If it is not, inform the cath lab.
The pump will automatically adjust the timing. Do not manually adjust the augmentation or
timing.
The pump will automatically choose pressure or ECG for the trigger.
A rounded balloon pressure waveform could imply a kink in the balloon.
Creation Date: 15 October 2023
Creation Date: 15 October 2023
Ridgeview Ambulance Protocols
Critical Care Protocols
Protocol CC0005
PARALYZATION FOR MECHANICALLY VENTILATED PATIENTS
CC0005 - PARALYZATION FOR MECHANICALLY VENTILATED PATIENTS
Purpose
To ensure patient and staff safety during transport of an adequately sedated adult patient, who is being
mechanically ventilated via endotracheal tube that has been previously confirmed to be in an appropriate
position
This is NOT a mandatory action that needs to be taken on all intubated patients, rather, a tool available when
needed for appropriate indications
Indications
Possible scenarios when paralytics may be required include (but are not limited to):
Improving ventilator synchrony (e.g. patient is “bucking”/resisting ventilations, or patient is over-breathing
ventilator settings)
If there is a persistent risk of ETT dislodgement despite appropriately dosed sedation
This will be required even if patient is showing no signs of distress
Additional information
Patients experiencing their paralysis (awareness of paralysis) is a NEVER EVENT – it should never occur and must be
avoided in every instance. It is imperative that effective sedation is given during neuromuscular blockage to avoid
awareness of paralysis.
PATIENTS WEIGHT MUST BE ENTERED IN KILOGRAMS
Creation Date: 15 October 2023
Creation Date: 15 October 2023
Ridgeview Ambulance Protocols
Critical Care Protocols
Protocol CC0006
AMBULANCE TRANSFERS REQUIRING A THIRD PERSON
CC0006 - AMBULANCE TRANSFERS REQUIRING A THIRD PERSON
Purpose: To assure adequate resources are available to provide safe care during interfacility transport.
Consideration/requirement criteria for needing addtional personnel:
Considerations:
Any patient requiring a 2:1 staff ratio to maintain stability.
Paramedic requests assistance based on patient's needs.
Hypotension requiring active titration of multiple vasopressors.
Suspected or imminent cardiovascular collapse.
Requirements:
Invasive pressure monitoring required:
Patient with an arterial line - requires a qualified RN or paramedic
Patient with a pulmonary artery catheter - requires a qualified RN
*If determined additional staff is needed for transport and unable to obtain, consider critical care transport or
air for transport.
Procedural Steps:
Unit staff advises dispatch of critically ill patient transfer and the potential "need for additional staff"
(meets one of the above consideration/requirement criteria).
- Dispatch gives estimated time of paramedic crew arrival to unit staff and deploys crew and paramedic
supervisor (if available) to patient location for team huddle.
Charge RN (or delegated to HUC) notifies the rest of the team member of huddle time (see checklist for 'who'
should huddle).
EMS staff and care team huddle and run checklist to discuss patient and need for additional staff for transport
based on the above consideration/requirement criteria
Unit staff secures and/or requests additional transport medications from pharmacy based on anticipated need
(minimum transport 45 minutes).
If it is determined that additional staff is required, the care team will quickly determine the most appropriate
team member to accompany the ambulance staff during transport.
- i.e., RN, RT, MD, Paramedic Supervisor, ED Tech, EMT etc.
When - to be used when a critically ill patient is being transported out of Ridgeview by the Ridgeview paramedic
team. (i.e. EDs, CICU, prep/recovery)
Who - bedside RN, paramedic team, charge RN, nursing supervisor, pharmacy (via phone at night), RT as needed (i.e.
patient vented or requires BiPAP), provider as appropriate
Where - team huddle at patient bedside
What - review below checklist items to determine what is needed for tranpsort
▢
Summary of patient/condition
▢
Vital signs and overall stability
▢
Current medication infusions, dose/rate
▢
Estimated transport time
▢
Estimate of infusion volume needed for transport
RN to obtain more medication for transport, as needed
Definition: Rapid Sequence Airway management utilizes the rapid sequential administration of a sedative and a paralytic
agent to facilitate intubation or placement of a supraglottic airway.
Personnel: This protocol is only for authorized manager or supervisor use. RSA medications may only be utilized under
the direction of Ridgeview Ambulance manager or supervisor. At least one other paramedic, plus one EMT or second paramedic,
must be on scene to assist with medication administration. Airway management (intubation) must be performed by the manager or
supervisor, not the assisting paramedic.
Indications:
Inability to oxygenate or ventilate
Impending airway compromise
Inability to manage airway due to combativeness, gag reflex or jaw clenching
Contraindications:
Factors increasing the likelihood of intubation failure
Major facial or laryngeal trauma
Limited jaw opening or cervical mobility in an otherwise flaccid patient
Distorted facial or airway anatomy
Upper Airway obstruction
Cardiac arrest state
Lack of any required equipment or personnel
Inability or achieve proper patient access and/or positioning
Caution:
Suspected DKA with spontaneous hyperventilation even with decreased LOC
Morbid obesity
Equipment:
Charged Video Laryngoscope with recording ON
Bougie
Appropriate size ETT with syringe attached and next size down.
Tube holder
Alternate airway devices (OPA/NPA, BVM, SGA)
Suction (two sources) with Ducanto available
Induction and paralytic agents drawn up with confirmed dose
Continuous ETCO2 monitor ready
NRB face mask and NC for pre and apneic oxygenation.
Ensure adequate personnel and equipment. Complete Pre-Procedure checklist
Include plan for difficult airway using HEAVEN criteria (see below)
Pre oxygenate with 100% O2
Place NC first with high flow O2
Conscious with adequate respirations apply NRB facemask and high flow
Unconscious or ineffective respiratory efforts require BVM ventilation with high flow O2 +/- PEEP
If adequate oxygenation/ventilation with BVM and airway adjunct or SGA DO NOT proceed with RSA
Obtain pre procedure vital signs, monitor ECG, SpO2
Identify patients in shock or peri-arrest state and provide fluid resuscitation and push dose epi if needed
Delayed RSA is preferred when able for patients in shock
Maintain inline cervical spine stabilization for known or suspected traumatic injury
Open the front portion once paralyzed while providing manual stabilization
Ensure optimal position
Obese patients may require extensive head/upper thorax elevation (ramping) to achieve ear-sternal notch
alignment
DO NOT proceed until adequate position is achieved
Draw up appropriate medications after confirming dose
Set ventilatory rate/tidal volume to achieve ETCO2 of 35-45 mm Hg
If concerns for preceding severe acidosis (Kussmaul or RR > 24) attempt to match the patients pre-procedure minute
ventilation and target ETCO to 20-30 mmHg
Assess for hypotension
Administer fluids and utilize push dose epi if not fluid responsive.
Consider repeat paralytic dose for long transport
<>Vecuronium<> 0.1mg.kg IV/IO if rocuronium is not available
Avoid if possible for status epilepticus.
Consider DOPES mnemonic for difficult ventilation:
Displacement: Did the ETT dislodge? Check end tidal, verify with direct visualization
Obstruction: ETT blocked by a foreign body or blood clot? Attempt suctioning
Pneumothorax: Check tube depth to verify no right main stem intubation (more common than pneumothorax,
verify tube depth is appropriate). Consider needle decompression if suspected tension pneumothorax
Equipment: Is your equipment functioning properly? End tidal line clogged, is oxygen valve running and
bag connected, sat probe, etc.
Stacked breaths: Common in obstructive disease! If it is difficult to ventilate, consider disconnecting the
bag and performing manual exhalation
If using rescue airway (SGA) consider change over bougie if inadequate SGA function
The HEAVEN criteria airway management checklist must be completed prior to all RSI airway management. Each individual
portion of the checklist requires documentation in the ePCR narrative.
Note: Our video Laryngoscope can be used in a Direct Laryngoscopy (DL) fashion like a standard Mac blade or a video
laryngoscope using the attached screen (VL)
H - Hypoxemia DL is faster if straightforward. VL maybe faster with anatomic difficulty.
E - Extremes of Size Extremely large patient: VL (out-to-in) —> DL (in-to-out) if not recognized. Extremely
small patient: DL with straight blade.
A - Anatomic Disruption/Obstruction VL (out-to-in) —> DL (in-to-out) if not recognized. DL if
bloody.
V - Vomit/Blood/Fluid DL with lift. Suction-Assisted Laryngoscopy and Airway Decontamination
(SALAD).
E - Exsanguination DL is faster. VL with anatomic difficulty.
N - Neck Mobility/Neurologic Injury Gentler VL.
Important: When using VL with a bougie it is CRITICAL to physically use the blade as you would with standard
DL. Without the airway/visual axis alignment the bougie is unlikely to enter the glottic opening and go through
the chords.
Creation Date: 15 May 2024
Creation Date: 15 May 2024
Ridgeview Ambulance Protocols
Critical Care Protocols
Protocol CC0008
Critical Care Medications - Vasopressors and Inotropes
Concentration
1600 mcg/mL
Dose & Administration
Usual range 0-20 mcg/kg/min
Initial Rate: 5 mcg/kg/min or per provider discretion
Titrate by 1 mcg/kg/min every 5 minutes to achieve target parameters
Maximum rate: 20 mcg/kg/min
Monitoring
Blood pressure and heart rate every 15 minutes
Rates vary based on patient weight.
Concentration
2000 mcg/mL
Dose & Administration
Usual range 0-20 mcg/kg/min
Initial Rate: 2 mcg/kg/min or per provider discretion
Titrate by 2 mcg/kg/min every 5 minutes to achieve target parameters
Maximum rate: 20 mcg/kg/min
Monitoring
Blood pressure and heart rate every 15 minutes
Rates vary based on patient weight.
Concentration
4 mcg/mL
Dose & Administration
Usual range 0-15 mcg/min
Initial Rate: 2 mcg/min or per provider discretion
Titrate by 1 mcg/min every 5 minutes to achieve target parameters
Maximum rate: 15 mcg/min; may exceed maximum per MD discretion to reach target
parameters
Monitoring
Blood pressure and heart rate every 15 minutes
Epinephrine Dose (mcg/min)
Rate (mL/hr)
Epinephrine Dose (mcg/min)
Rate (mL/hr)
1
15
9
135
2
30
10
150
3
45
11
165
4
60
12
180
5
75
13
195
6
90
14
210
7
105
15
225
8
120
Infusion Rate Calculation (mL/hr) = (1mL/4mcg)*(mcg/min)*60 min
Concentration
16 mcg/mL
Dose & Administration
Usual range 0-30 mcg/min
Initial Rate: 2 mcg/min or per provider discretion
Titrate by 1 mcg/min every 5 minutes to achieve target parameters
Maximum rate: 30 mcg/min; may exceed maximum per MD discretion to reach target
parameters
Monitoring
Blood pressure and heart rate every 15 minutes
Norepinephrine Dose (mcg/min)
Rate (mL/hr)
Norepinephrine Dose (mcg/min)
Rate (mL/hr)
1
3.8
16
60
2
7.5
17
63.8
3
11.3
18
67.5
4
15
19
71.3
5
18.8
20
75
6
22.5
21
78.8
7
26.3
22
82.5
8
30
23
86.3
9
33.8
24
90
10
37.5
25
93.8
11
41.3
26
97.5
12
45
27
101.3
13
48.8
28
105
14
52.5
29
108.8
15
56.3
30
112.5
Infusion Rate Calculation (mL/hr) = (1 mL/16mcg)*(mcg/min)*60 min
Concentration
100 mcg/mL
Dose & Administration
Usual range 0-180 mcg/min
Initial Rate: 20 mcg/min or per provider discretion
Titrate by 10 mcg/min every 5 minutes to achieve target parameters
Maximum rate: 180 mcg/min; may exceed maximum per MD discretion to reach target
parameters
Monitoring
Blood pressure and heart rate every 15 minutes
Phenylephrine Dose (mcg/min)
Rate (mL/hr)
Phenylephrine Dose (mcg/min)
Rate (mL/hr)
20
12
110
66
30
18
120
72
40
24
130
78
50
30
140
84
60
36
150
90
70
42
160
96
80
48
170
102
90
54
180
108
100
60
Infusion Rate Calculation (mL/hr) = (1 mL/100mcg)*(mcg/min)*60 min
Concentration
0.2 units/mL
Dose & Administration
Target dose: 0.04 units/min for septic shock
Initial Rate: 0.02 units/min
Titrate by 0.01 units/min every 10 minutes to dose of 0.04 units/min
Maximum rate: 0.04 units/min
Monitoring
Blood pressure and heart rate every 15 minutes
Vasopressin Dose (mcg/min)
Rate (mL/hr)
Vasopressin Dose (mcg/min)
Rate (mL/hr)
0.01
3
0.03
9
0.02
6
0.04
12
Critical Care Medications - Antihypertensives and Vasodilators
Concentration
0.5 mg/mL
Dose & Administration
Usual range 0-21 mg/hr
Initial Rate: 1 mg/hr
Titrate by 2 mg/hr every 90 seconds to achieve target parameters. As BP approaches
target, increase slowly by 0.5-1 mg/hr every 5 minutes until goal is achieved.
Maximum rate: 21 mg/hr
Do not mix with or administer in same line as other medicaitons.
Monitoring
Blood pressure and heart rate every 15 minutes
Clevidipine Dose (mcg/min)
Rate (mL/hr)
Clevidipine Dose (mcg/min)
Rate (mL/hr)
1
2
12
24
2
4
13
26
3
6
14
28
4
8
15
30
5
10
16
32
6
12
17
34
7
14
18
36
8
16
19
38
9
18
20
40
10
20
21
42
11
22
Concentration
10 mg/mL
Dose & Administration
Usual range 0-300 mcg/kg/min
Initial Rate: 25 mcg/kg/min
Titrate by 25 mcg/kg/min every 10 minutes to achieve target parameters
(blood pressure and heart rate)
Maximum rate: 300 mcg/kg/min
Monitoring
Blood pressure and heart rate every 15 minutes
Rates vary based on patient weight.
Concentration
0.1 mg/mL
Dose & Administration
Usual range 0-15 mg/hr
Initial Rate: 5 mg/hr
Titrate by 2.5 mg/hr every 5 minutes to achieve target parameters
Maximum rate: 15 mg/hr
Monitoring
Blood pressure and heart rate every 15 minutes
Nicardipine Dose (mcg/min)
Rate (mL/hr)
Nicardipine Dose (mcg/min)
Rate (mL/hr)
1
10
9
90
2
20
10
100
3
30
11
110
4
40
12
120
5
50
13
130
6
60
14
140
7
70
15
150
8
80
Infusion Rate (ml/hr) = Dose (mg/hr) / 0.1 mg
Concentration
200 mcg/mL
Dose & Administration
Usual range 0-100 mcg/min
Initial Rate: 5 mcg/min
Titrate by 5 mcg/min every 5 minutes to achieve target parameters
Maximum rate: 100 mcg/min
Monitoring
Blood pressure and heart rate every 15 minutes
Critical Care Medications - Antiarrhythmics
Concentration
1.8 mg.ml
Dose & Administration
Usual Infusion Dose: Usually following bolus dose, 1 mg/min for 6 hours, followed
by 0.5 mg/min for 18 hours.
Usual Rate: 0.5 - 1 mg/min
Premixed bags require a 0.2 micron filter
Monitoring
Blood pressure, heart rate and rhythm every 15 mintes
Critical Care Medications - Pain and Sedation
Concentration
10 mcg/mL
Dose & Administration
Usual range 0-250 mcg/hr
Initial Rate: 25 mcg/hr
Titrate by 25 mcg/hr every 10 minutes as needed to achieve target pain or RASS
goal
Maximum rate: 250 mcg/hr. If patient is requiring more than max rate ordered,
please contact the provider for additional orders.
Monitoring
Pain level and sedation level (RASS) Blood pressure
Concentration
4 mcg/mL
Dose & Administration
Usual range 0-1.5 mcg/kg/hr
Initial Rate: 0.2 mcg/kg/hr
Titrate by 0.1 mcg/kg/hr every 10 minutes as needed to achieve target RASS
goal
Maximum rate: 1.5 mcg/kg/hr. If patient is requiring more than max rate ordered,
please contact the provider for additional orders.
Can cause bradycardia
Monitoring
Sedation level (RASS) Blood pressure and heart rate
Rates vary based on patient weight.
Concentration
1 mg/mL
Dose & Administration
Usual range 0-10 mg/hr
Initial Rate: 1 mg/hr or per provider
Titrate by 1 mg/hr every 5 minutes as need too achieve target RASS goal
Maximum rate: 10 mg/hr. If patient is requiring more than max rate ordered,
please contact the provider for additional orders.
Monitoring
Sedation level (RASS) Blood pressure
Concentration
10 mg/mL
Dose & Administration
Usual range 0-80 mcg/kg/min
Initial Rate: 10 mcg/kg/min or per provider
Titrate by 10 mcg/kg/min every 5 minutes as need to achieve target RASS
goal
Maximum rate: 80 mcg/kg/min. If patient is requiring more than max rate
ordered, please contact the provider for additional orders.
Monitoring
Sedation level (RASS) Blood pressure
RASS value definitions (Richmond Agitation
and Sedation Scale)
+4
= Combative
overtly comabtive, violent, immediate danger to staff
+3
= Very Agitated
Pulls or removes tube(s) or catheter(s), aggressive
If you are called by a patient or family member for a “Condition H”, get the patient’s room number and give that
information to the nursing supervisor (or duty manager/director during the day.)
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
ECMO Auto Launch
Rural ECPR
Dispatch Proceedure - Confirmed Cardiac Arrest
Dispatch crew and assist caller per normal proceedure.
For patients ≤ 76 y/o or unknown, Request LL3 to established LZ for Rural ECPR.
Establish TAC channel and advise crew.
Must be responding from Blaine, Willmar or within close proximity i.e. metro hospitals.
If not ressponding from above locations cancel and advise crew.
Alarm sounding / visible smoke, drills -
(remember to call Wound and Hyperbaric at 35178 for drills)
“Fire Response Stage III” (location)
Flames and smoke
Call Maintenance
Call or Vortex Alert Supervisor
Announce to Security via radio
Include Location
Call CCSO for Fire Department Response
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
Hazardous Spill
Hazardous Spill
Announce 3 times on Overhead Emergency Page
“Spill Response Stage I, (location)”
“Spill Response Stage II, (location)”
“Spill Response Stage III, (location)”
Call Facilities Engineer
Announce to Security via radio
Call Administration for Stage 2 or 3
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
Manager / Supervisor / Medical Director Notification Criteria
MANAGER / SUPERVISOR / MEDICAL DIRECTOR NOTIFICATION CRITERIA
Purpose :
Managers, Supervisors and Medical Directors should be made aware, via Vortex of high acuity, multiple rig response
and special operations type incidents, when EMS has been activated. In addition, pertinent follow up information
should be sent to the manager and supervisor group when applicable.
Process :
The following incidents below should activate the Manager/Supervisor group And Medical Directors via vortex. Include the
incident nature, address, and any pertinent details. In the event vortex is down, the on-call manager should be notified
via phone, the on-call manager will then alert the other managers and supervisors as necessary.
Manager/Supervisor/Medical Director Notification Criteria :
The transporting crew will notify dispatch that they are transporting to the U of M with a “Refractory V-fib”
patient and ask for notification of the team.
Dispatch will -
Notify Dr. Yannapoulos on his cell phone at 612-616-7575.
IF HE DOES NOT ANSWER, RETRY EVERY 5
MINUTES!
Advise that we are coming in with a “Persistent V-Fib cardiac arrest.”
Give the ETA.
Tell the crew to contact WMRCC per usual routine!
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
Rapid Response Team (RRT)
Rapid Response Team (RRT)
When an RRT is requested by staff -
Non-Emergency Overhead page 3 times.
Send a Vortex Alert to the RRT group.
Include the term RRT.
Whether the patient is adult or pediatric.
The room number.
You MAY be requested to page the Hospitalist as well.
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
RSMC Lockdown
RSMC Lockdown
Immediately call Sibley County dispatch and advise them of lockdown.
Call 507-964-8415; attempt to get further information
If you are able to get information, update Sibley County dispatch.
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
Security Problem
Security Problem
Announce 3 times on Overhead Emergency Page -
“Safety Response Stage II, (location)”
Multiple people or out of control situation
“Safety Response Stage III, Leadership to (location)”
Security issue involving whole facility
Call CCSO for help.
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
Sepsis Team
Sepsis Team
The ED will decide if a Sepsis Team response is necessary based on crew request or patient exam.
If the ED requests it, send a Vortex Alert to -
The “Sepsis Team”
The Hospitalist
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
Stroke Team
Stroke Team
ED RN or HUC will contact dispatch for Stroke Code paging need. You will page in one of two ways:
Walk in stroke code activations will start in ED Triage called by RN, they will be announced
as “Stroke Code Triage.”
EMS pre arrival strokes will be announced as “Stroke Code ED.”
PLEASE continue to fill out Code forms and send to Kerri Specht. The MR# is only required for inpatient activations. It is
not an issue if included on all, but you don’t need to on all the other activations.
12 March 2023
12 March 2023
Ridgeview Dispatch Protocols
Trauma Team
Trauma Team
The crew will call the ED and describe the TTA patient. The ED will then call “88” and inform dispatch whether the
TTA is Level 1 or Level 2.
IF RMC TTA: Overhead page “Trauma Team, Level xxx; ETA xxx Minutes” DO NOT VORTEX
IF TTMC TTA: The HUC announces the TTA and sends the Vortex Alert, Dispatch advises 8350
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
Weather
Weather
Announce 3 times on Overhead Emergency Page (Hospital AND TTMC) -
Advise supervisor of current or pending conditions before announcing Stage 2 or 3
(must get Supervisor / Administration approval for Stage 2 / 3.)
“Weather Response Stage I”
Severe Thunderstorm Warning and / or Tornado Watch.
“Weather Response Stage II”
Severe Thunderstorm Warning (winds >70 mph) or Tornado
Warning.
“Weather Response Stage III”
Damage occurs to facility.
Perform Lynx Alert -
Name all involved counties with RMC locations:
Carver
Hennepin
Le Sueur
McLeod
Scott
Sibley
Wright
Alert all ambulance out bases.
Remind 8300 to distribute radios for Stage 1 and Stage 2.
For Stage II after maintenance hours -
Close Fire Doors
Activate Generator
At end of WEATHER RESPONSE, send "All Clear" over the Lynx update.
2 January 2017
2 January 2017
Ridgeview Dispatch Protocols
Transfer
Transfer
20 Nov 2025 Transfer Criteria
A group of EMT’s that live within an hour of the south bases are interested in taking long distance transfers. It’s in
vortex as the South Transfer Group, and can be used when RLMC is sitting on a BLS transfer that can pend for 60 minutes.
17 May 2022
17 MaY 2022
Ridgeview Dispatch Protocols
Disgruntled Caller(s)
Disgruntled Caller(s)
Repetitive callers, who during the conversation it appears the person is unreasonable/irrational and not listening and is
stuck in a pattern of conversation that is cyclical; and or the person threatens, yells, screams, and or calls back
repeatedly in a harassment type way and tying up dispatch phone lines.
Follow the steps bellow.
Transfer the caller to the security phone
Have the security phone answered and place the caller on an open line
Mute the phone
Create an IT submission and request the callers number to be blocked
If request doesn’t get created in a reasonable period of time call Jason at 75037.
If he doesn’t answer or if you do not have a resolve within a reasonable period of time. Please call me (Vern).
20 March 2020
20 March 2020
Ridgeview Dispatch Protocols
Mental Health Stanby
Mental Health Stanby
For the time being this will only apply to areas covered by CCSD. We will start working on some of the other agencies to adopt
the same policy.
We will continue to respond to mental health standbys as we currently do.
After CCSD makes contact with the patient they will be put on a 5 minute timer to update RAS on the situation.
If we don't hear anything from CCSD at 10 minutes we will contact Carver Dispatch directly for an update.
The officers will clear our rig from standby under the following circumstances:
When the crisis team is making a scene response and/or initiating a virtual visit.
When the officer anticipates a prolonged scene time > 20-30 minutes.
If transport is required, we will be called back when the patient is ready to be transported.
17 March 2022
17 March 2022
Ridgeview Dispatch Protocols
Backfilling Belle Plaine and Le Sueur
Backfilling South PSA
With the southern portion of our service area getting busier, and having more and more instances of our BP and LS trucks out
simultaneously, we will be implementing slight modifications to our core coverage pattern to better keep the 169 corridor
covered. For the most part this will apply when 934 takes a transfer out of RLSMC, but may also be utilized if we are completely
out of rigs in the south and have adequate coverage in the north. If we are between 7 and 3 rig coverage we will be sending a
core truck to BP if no trucks are available in the south. We will not go below 2 rig in the core to cover BP. In rare instances
you may be asked to cover the south from Cologne based upon our coverage pattern in the north and/or other factors such as off
times etc… This is a work in process and will likely be further modified as we move forward.
17 November 2019
17 November 2019
Ridgeview Dispatch Protocols
DEPLOYMENT
EMT / Paramedic Crews are not separate; all crews should be treated the same.
Rigs Available
Chaska
Watertown
Waconia
Minnetrista
Minnewashta
Mayer
Norwood Young America
When in 4 rig (7a) we will use 284 as an E/W divider and anything east will be Chaska and west New Germany.
In 2 rig 284 will again be the divider and anything to the west will be Watertown and east Chaska.
Deployment Plan - 8 October 2019
Speed Code Reference
12 HI Trailer Court [ 12HI ]
212 Medical Center ANY CLINIC IN BUILDING [ 212 ]
Abbott Northwestern Hospital [ ANW ]
Adult Training & Rehab Center [ ATRC ]
Annandale CBHH [ ACBHH ]
Arlington Good Samaritan NH [ AGSC ]
Auburn Courts - Chaska [ AUBCRT ]
Auburn Homes - Waconia [ AUBW ]
Auburn Manor - Chaska [ AUBMNR ]
Belle Plaine Lutheran Home [ BPLH ]
Bethesda Hospital [ BETH ]
Bongards [ BNGRDS ]
Brown County Detox Center [ BCDC ]
Buffalo Hospital [ BUFH ]
Buffalo Lake Nursing Home [ BLNH ]
Byerlys (Chanhassen) [ BRLYS ]
Carris Health - Rice Memorial Hosptial Willmar [ CHWILL ]
Carver County Government Center [ CCGC ]
Carver County Jail [ CCJAIL ]
Catalyst Clinic - Watertown [ CTLST ]
Chanhassen Dinner Theater [ CHNDNR ]
Chaska Community Center [ CCOMCT ]
Chaska Heights Senior Living - Assisted [ CHSLA ]
Chaska Heights Senior Living - Independant [ CHSLI ]
Children's Health Care - Minneapolis - XER [ CHCM ]
Children's Health Care - St. Paul - XER [ CHCSP ]
Dakota Co Receiving Center [ DCRC ]
Emerald Crest [ ECV ]
Essentia Health - St. Joseph's Brainerd [ ESJ ]
Fairview Jonathon Clinic [ FVJON ]
Fairview Lakes Medical Center - Wyoming [ FVLKS ]
Fairview Northland Medical Center [ FVNRTH ]
Fairview Ridges Hosptial [ FVRIDG ]
Fairview Southdale Hosptial [ FVSDF ]
Fairview U of M East Bank - XER [ FVUM ]
Fairview U of M West Bank - XER [ FVRIVR ]
Fairview U of M Masonic Children's Hosptial - XER [ FVUMAM ]
First Street Center [ FSC ]
Gale Woods Farm Park [ GWFP ]
Garden House @ St. Mary's [ GH ]
Gillette Children's Hospital [ GIL ]
Glencoe Regional Health Services [ GRHS ]
Haven Homes [ HAVH ]
Hazeldon Treatement Center (Chaska) [ HAZ ]
Hazelton National Golf Course [ HAZEL ]
Hennepin County Detox [ HCMCDC ]
Hennepin County Medical Center [ HCMC ]
Howard Lake Good Samaritan [ HLGSC ]
Hutchinson Area Health Center [ HAHC ]
Kings Path Senior Living [ KPSL ]
Kohls (Chaska) [ CHKOHL ]
Lake Minnetonka Regional Park [ LMTRP ]
Lake Minnewashta Regional Park [ LMWRP ]
Lakeview Clinic - NYA [ LKVNYA ]
Lakeview Clinic - Waconia [ LKVWAC ]
Lakeview Clinic - Watertown [ LKVWT ]
Lakeview Hospital - XER [ LVH ]
Lakeview NH - Gaylord [ GLVNH ]
Lester Prairie Glencoe Clinic [ GCLPC ]
Lindenwood Apartments [ LNDN ]
Long Lake Nursing Home [ LLNH ]
Mayo Clinic Health System - Albert Lee [ MCAL ]
Mayo Clinic Health System - Austin [ MCAUS ]
Mayo Clinic Health System - Methodist Rochester [ MMR ]
Mayo Clinic Health System - Red Wing [ FVRW ]
Mayo Clinic Health System - St. Mary's Rochester [ SMH ]
Meeker County Memorial Hosptial [ MCMH ]
Mercy Hospital [ MERCY ]
Methodist Hospital - SLP [ METH ]
Mission Hills [ MISSION ]
Mocha Monkey (West Waconia) [ MMON2 ]
Monarch Estates - Delano [ GLCD ]
Monarch Estates - Excelsior [ GLCEXC ]
Mound Westonka High School [ MWHS ]
New Ulm Medical Center [ NUMC ]
North Memorial Medical Center [ NORTH ]
Oak Terrace Senior Living - Gaylord [ OAKT ]
Owatonna Hosptial [ OWA ]
Park Nicollet Clinic - Chanhassen [ PNMC ]
Peace Villa [ PVILLA ]
Prairie Care Chaska [ PCC ]
Prairie St. John's - Fargo [ PSJ ]
Presbyterian Homes [ PRESBY ]
Regina Memorial Hospital [ RMH ]
Regions Hospital [ REG ]
Ridgeview Clinic - Belle Plaine [ RVBPC ]
Ridgeview Clinic - Chanhassen [ RCC ]
Ridgeview Clinic - Delano [ RVDC ]
Ridgeview Clinic - Excelsior [ REXC ]
Ridgeview Clinic - Gaylord [ RVGC ]
Ridgeview Clinic - Howard Lake [ RHLC ]
Ridgeview Clinic - Spring Park [ RWTC ]
Ridgeview Clinic - Winsted [ RVW ]
Ridgeview Le Sueur Medical Center [ RVLS ]
Ridgeview Medical Center [ RMC ]
Ridgeview Medical Place [ RMP ]
Ridgeview Professional Bldg [ RPB ]
Ridgeview Sibley Medical Center [ RSMC ]
Shriner's Hospital [ SHRNRS ]
St. Gertrude's Health Center [ SGHC ]
St. Francis Regional Medical Center [ SFRMC ]
St. John's NE - XER [ STJ ]
St. Joseph's Hosptial - St. Paul - XER [ STJOES ]
St. Mary's NH - Winsted [ STMCC ]
St. Peter State Hosp/Mental Health [ SPCBHH ]
Stiftungsfest [ STIF ]
Summerwood of Chanhassen - 525 [ SUMRWD ]
Talheim Apts. [ TLHM ]
Target Chanhassen [ TRGTCH ]
Target Chaska [ TRGTCHS ]
Target Waconia [ TRGTWA ]
Trillium Assisted Living [ TRILL ]
Two Twelve Medical Center (ED ONLY) [ TTMC ]
United Hospital - XER [ UNITD ]
Unity Hospital [ UNITY ]
Valley Hospital at Hidden Lakes [ RGNCY ]
VAMC - Minneapolis [ VAHM ]
VAMC - St. Cloud [ VAHSTC ]
Victoria Care Center [ VCC ]
Waconia Event Center [ LKSD ]
Waconia Good Samaritan NH [ WGSC ]
Waconia Ice Arena [ WICE ]
Westview Acres [ WVA ]
Westwood Place [ WWOOD ]
Willmar Regional Treatment Center [ WRTC ]
Winthrop Good Samaritan Center [ WINGSC ]
Woodwinds Hosptial - Woodbury [ WOODW ]
Revision Date: 8 October 2019
Revision Date: 8 October 2019
Ridgeview Emergency Medical Services
Under Construction
Use your browsers back button to return to the page you were just on.


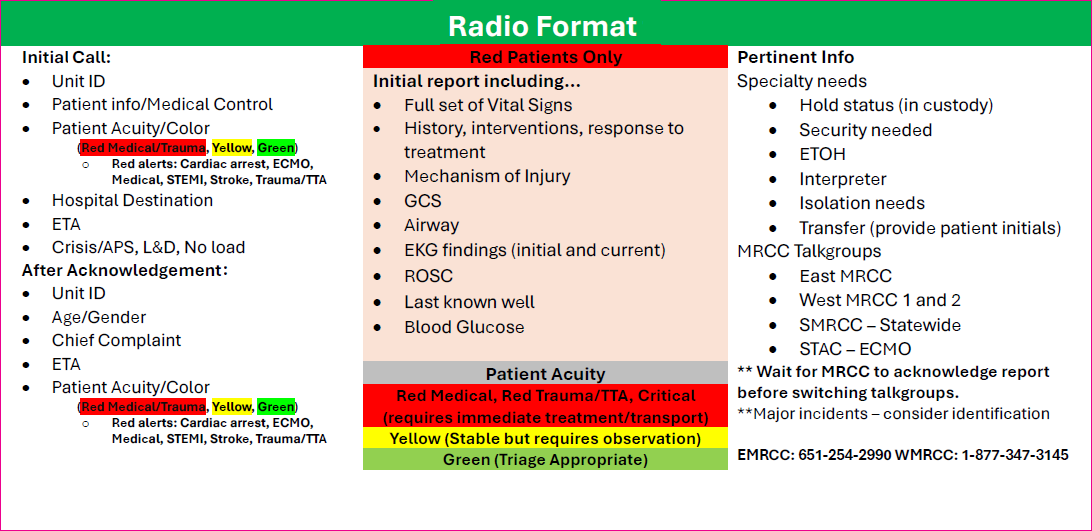
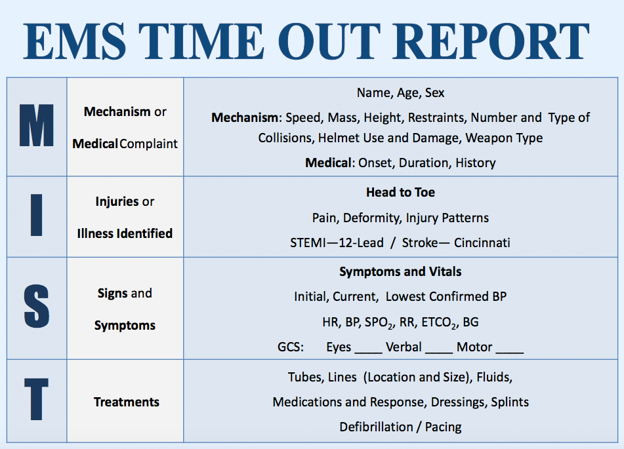
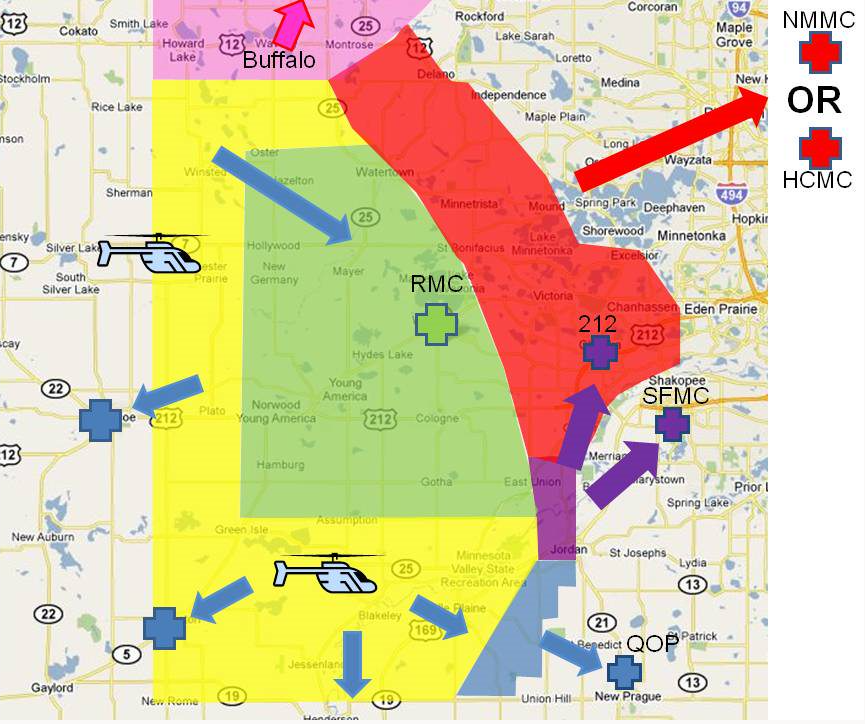


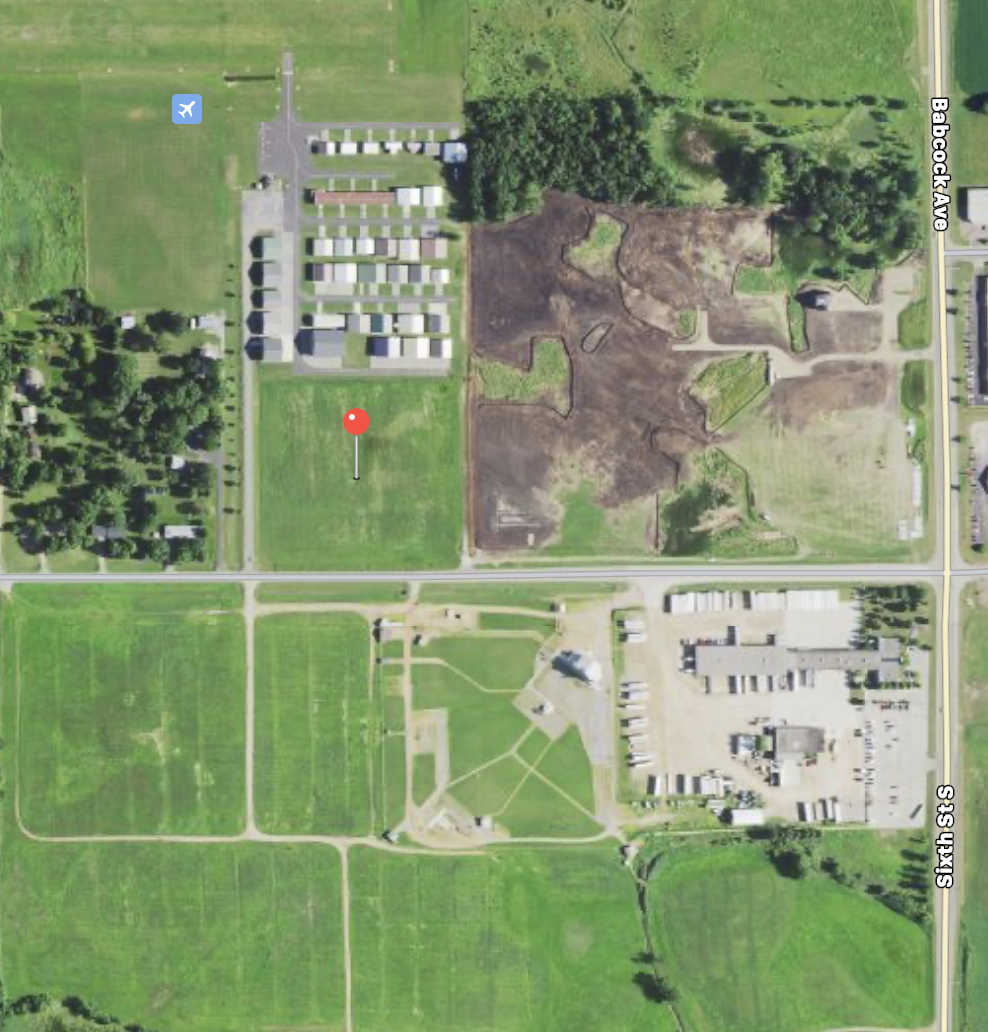


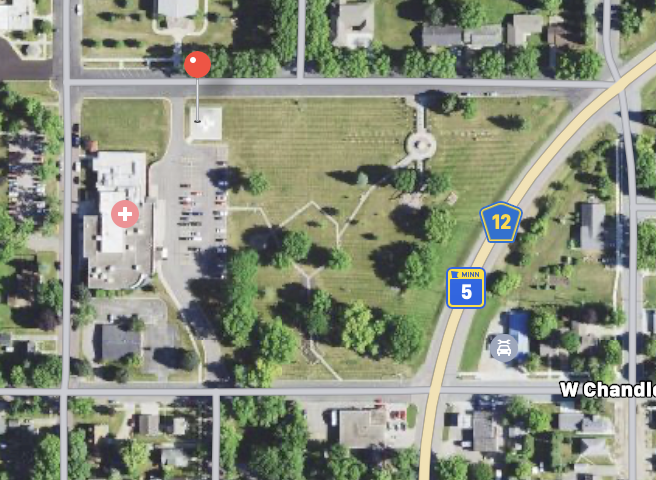








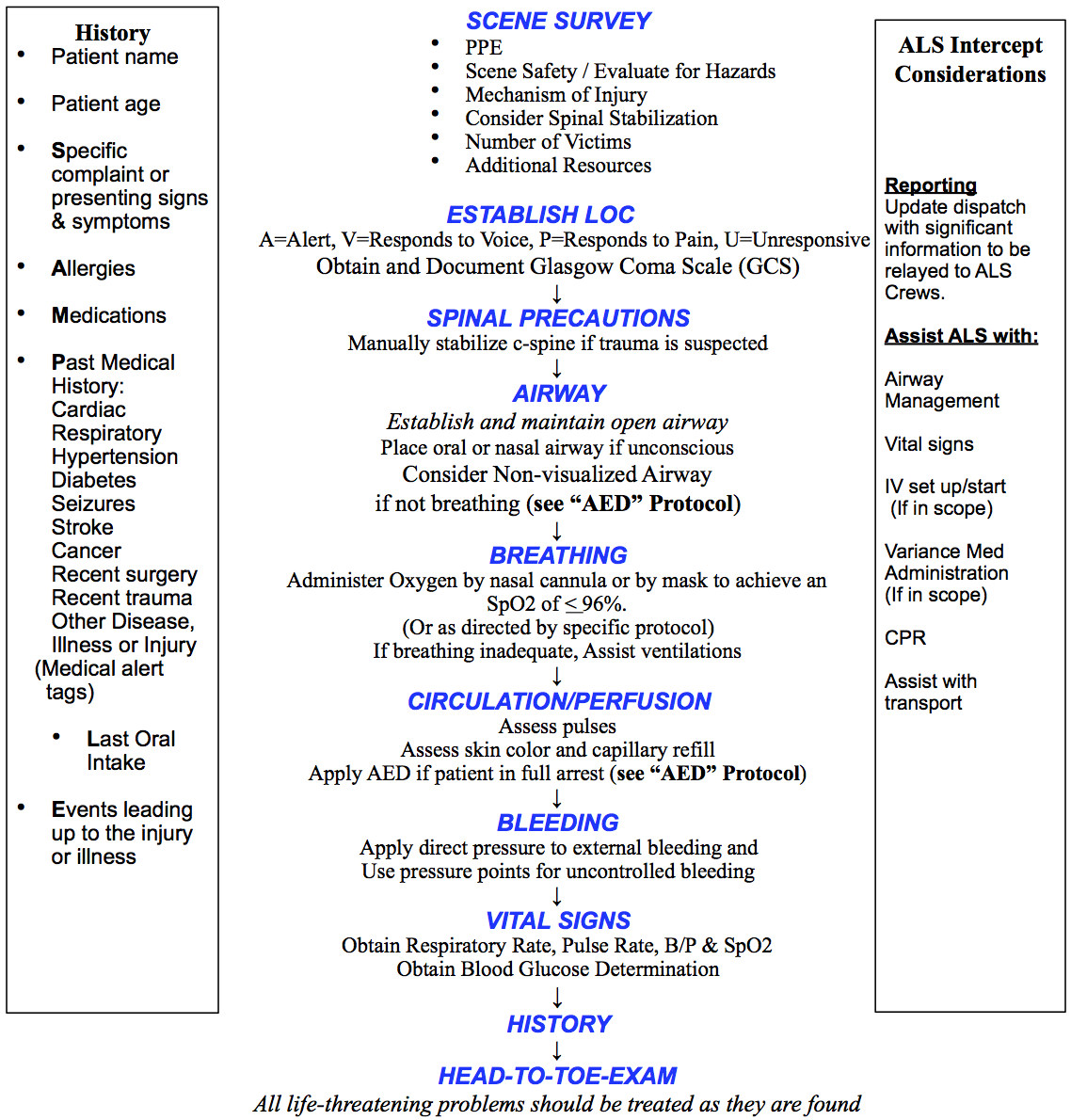
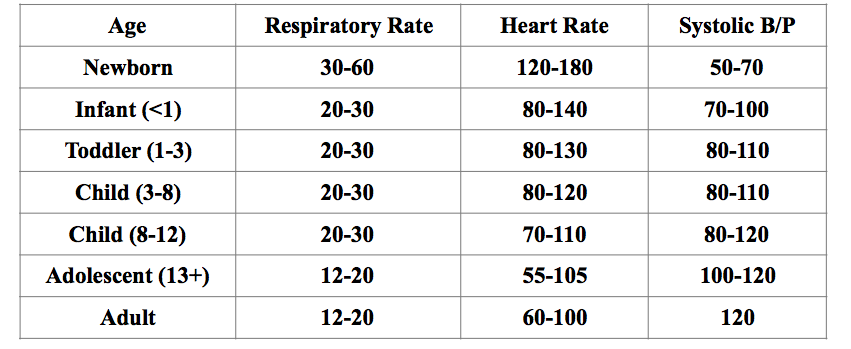
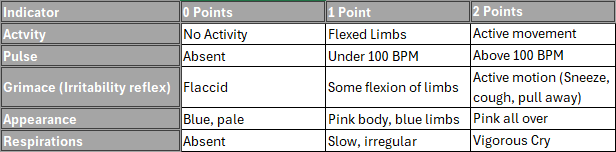
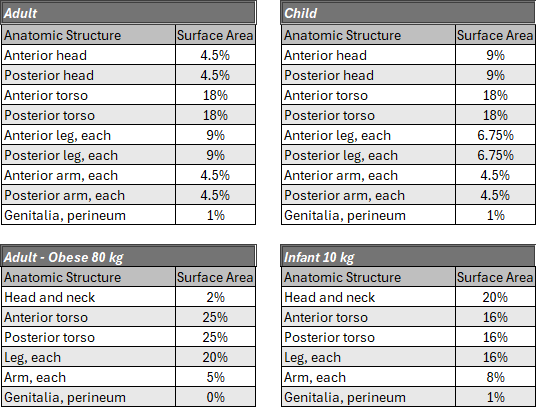
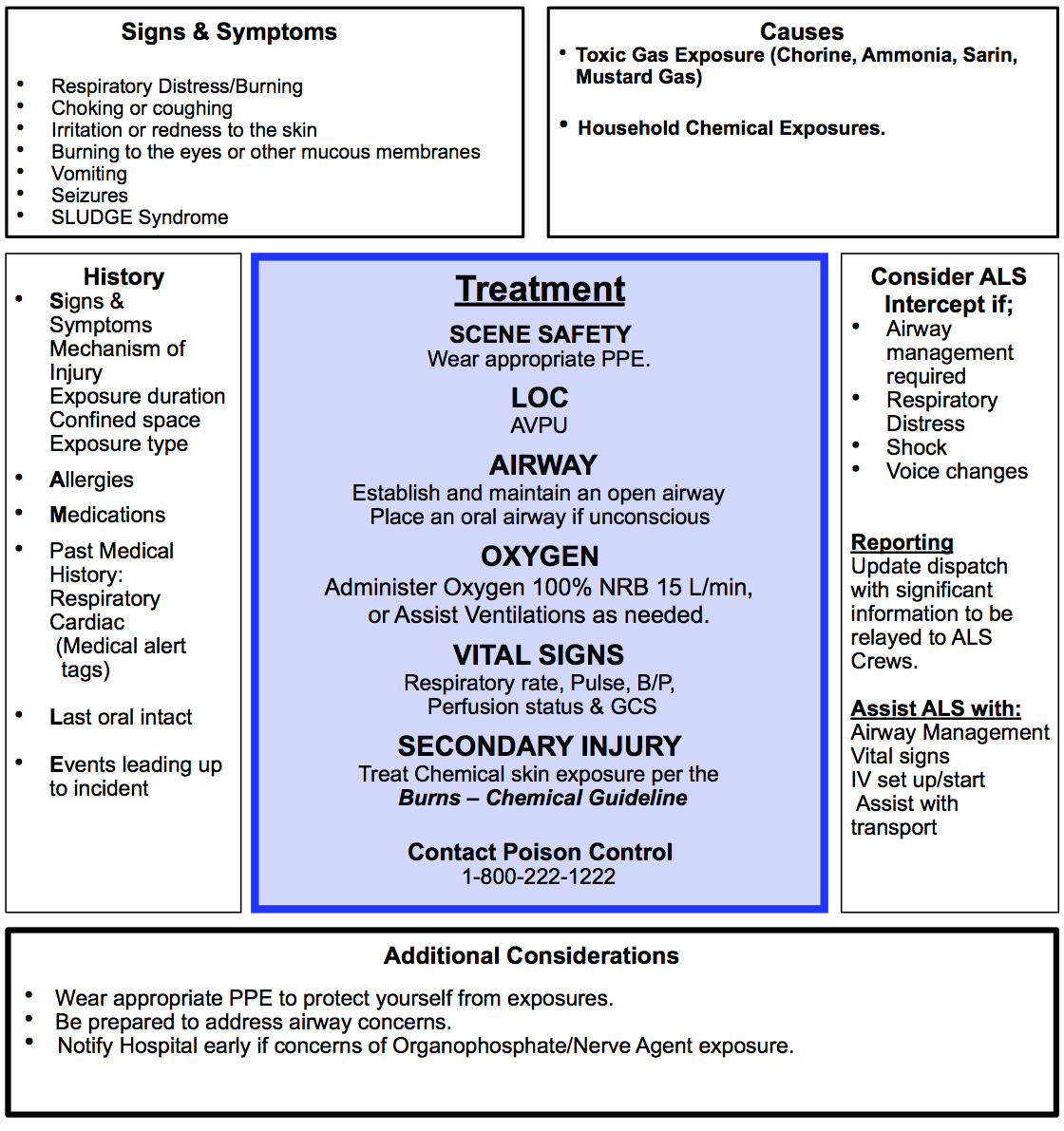
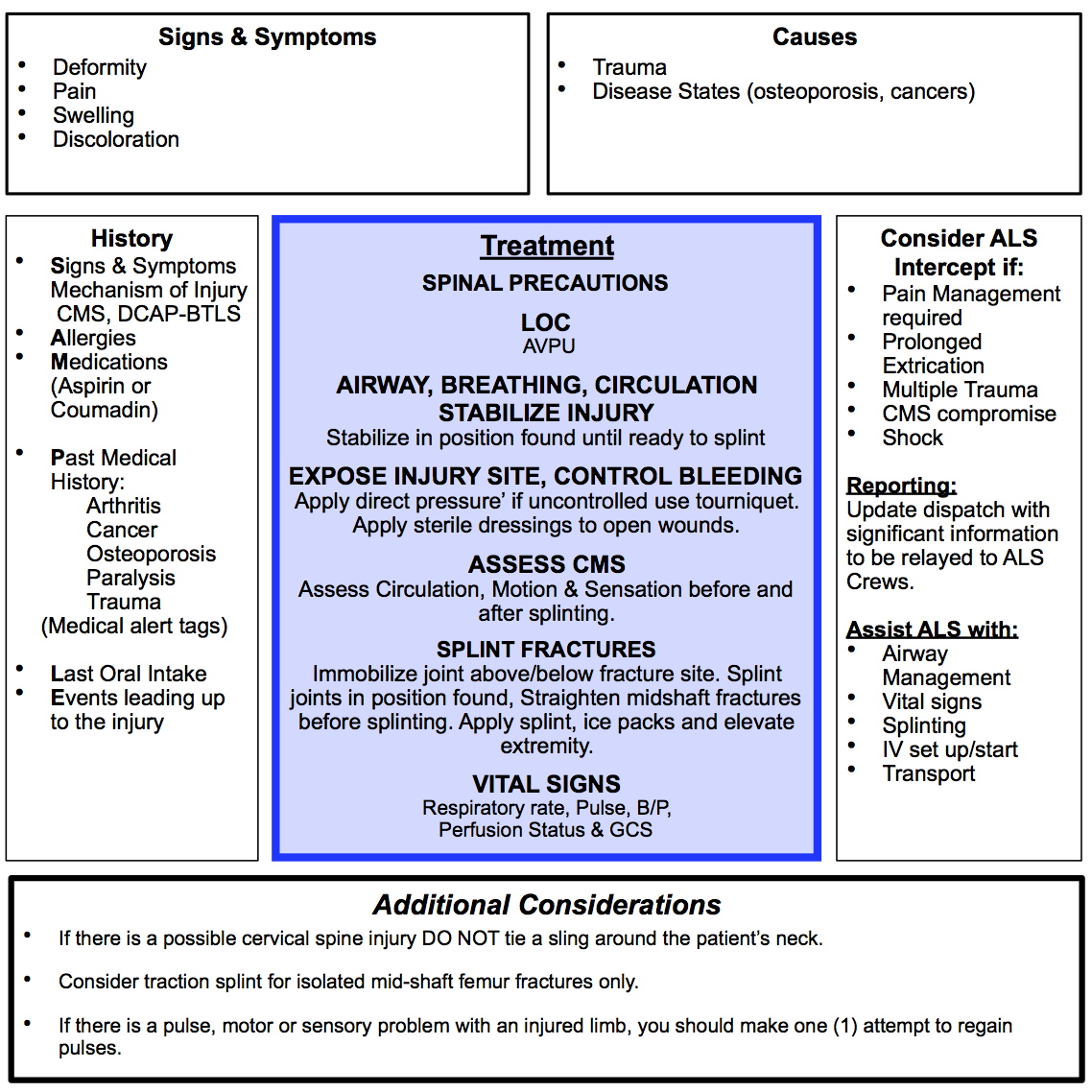
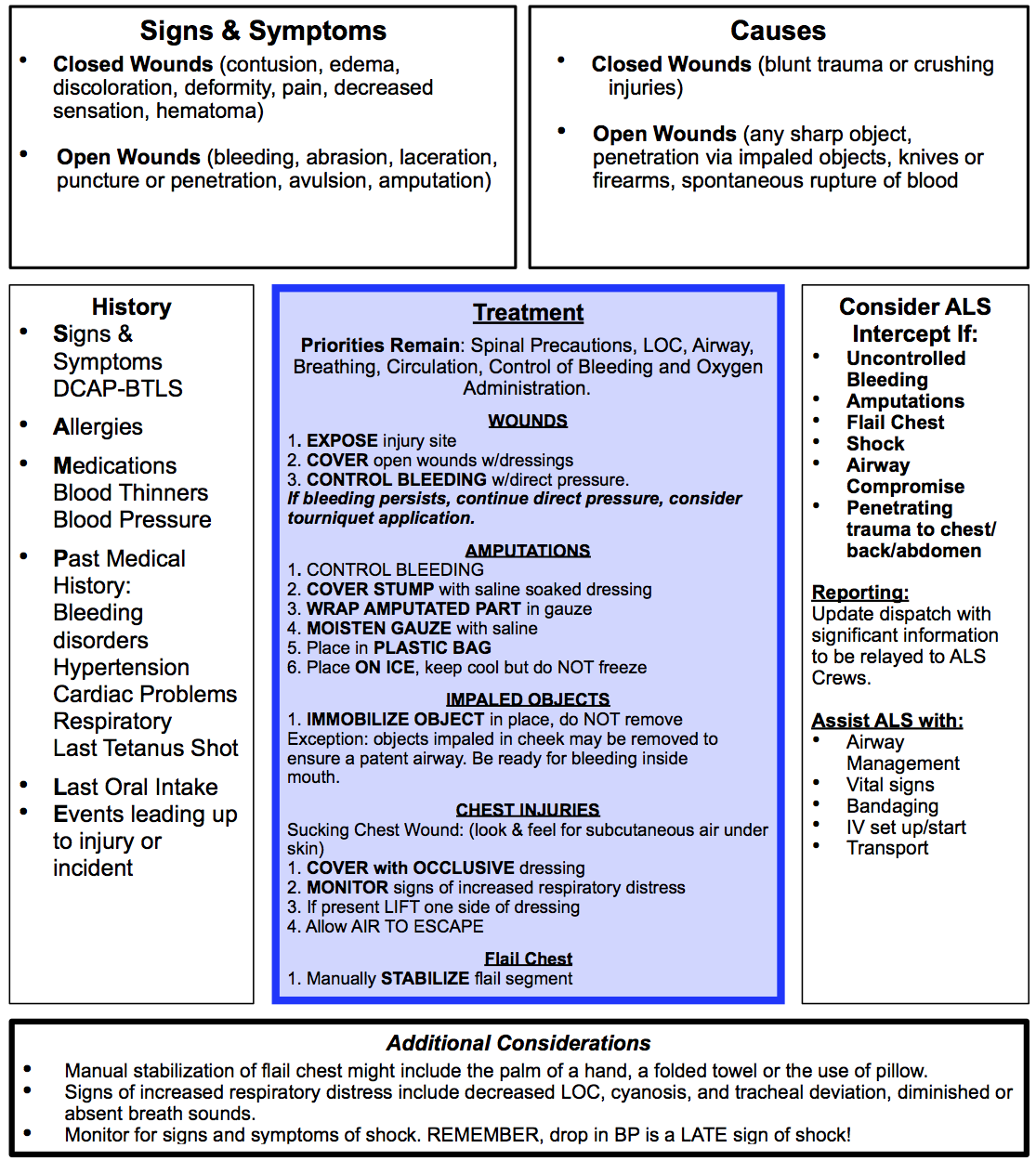
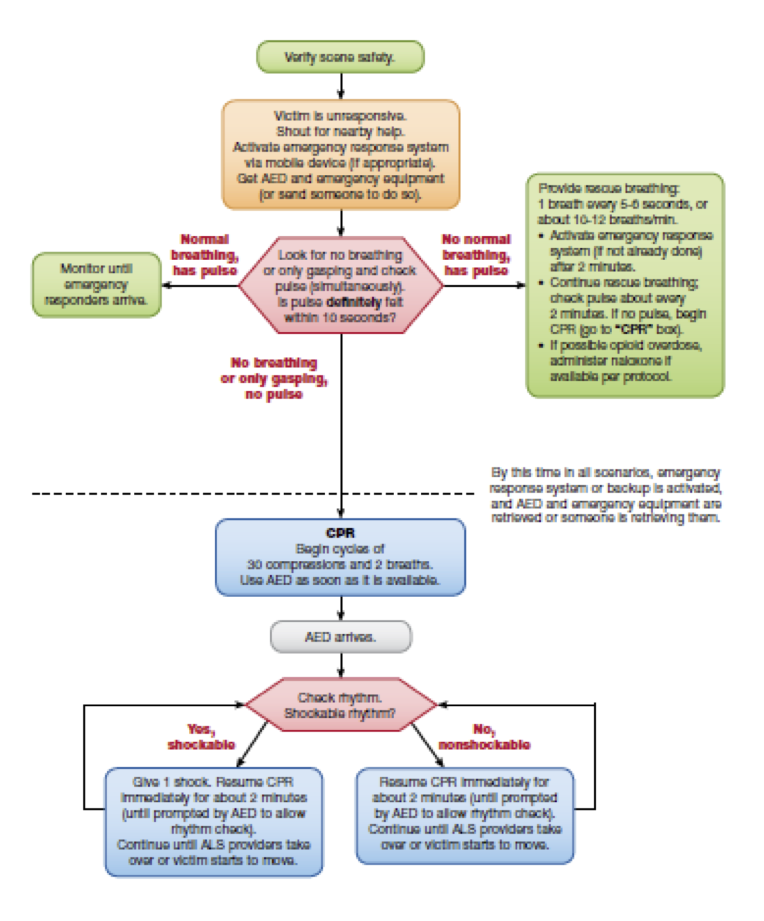
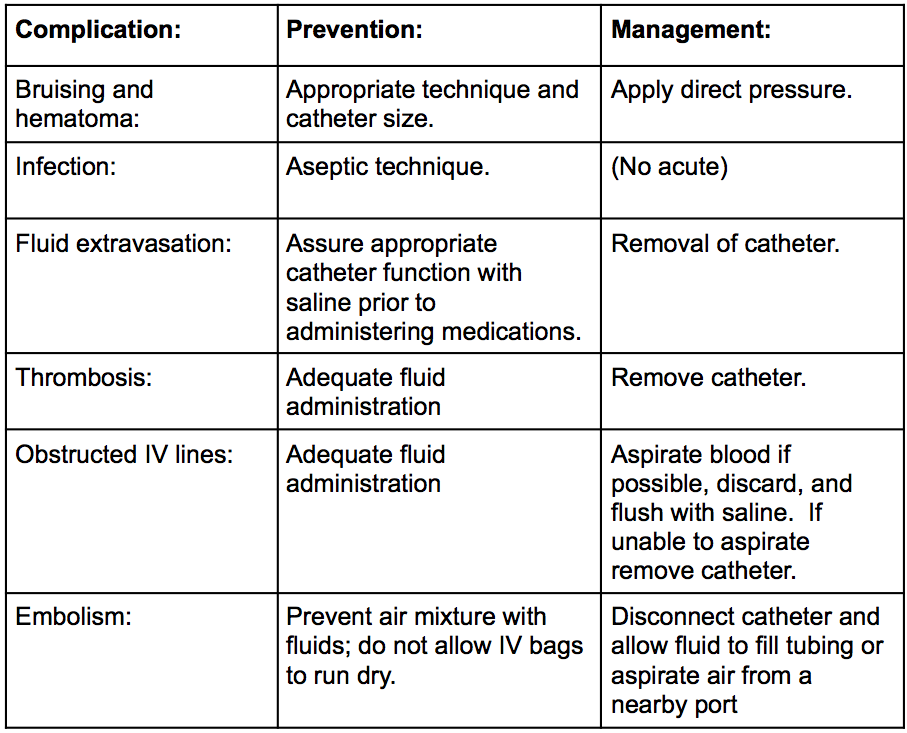
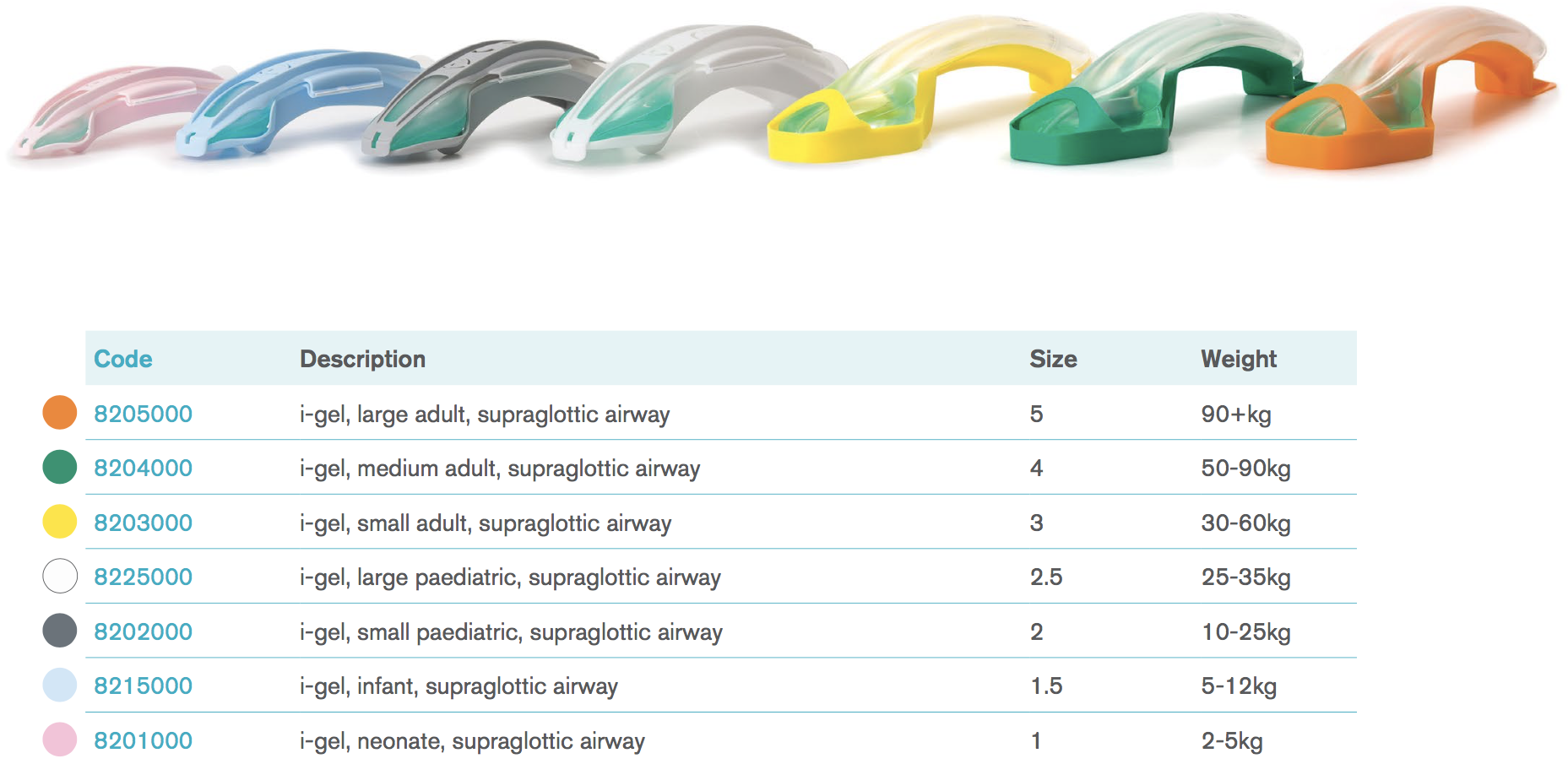
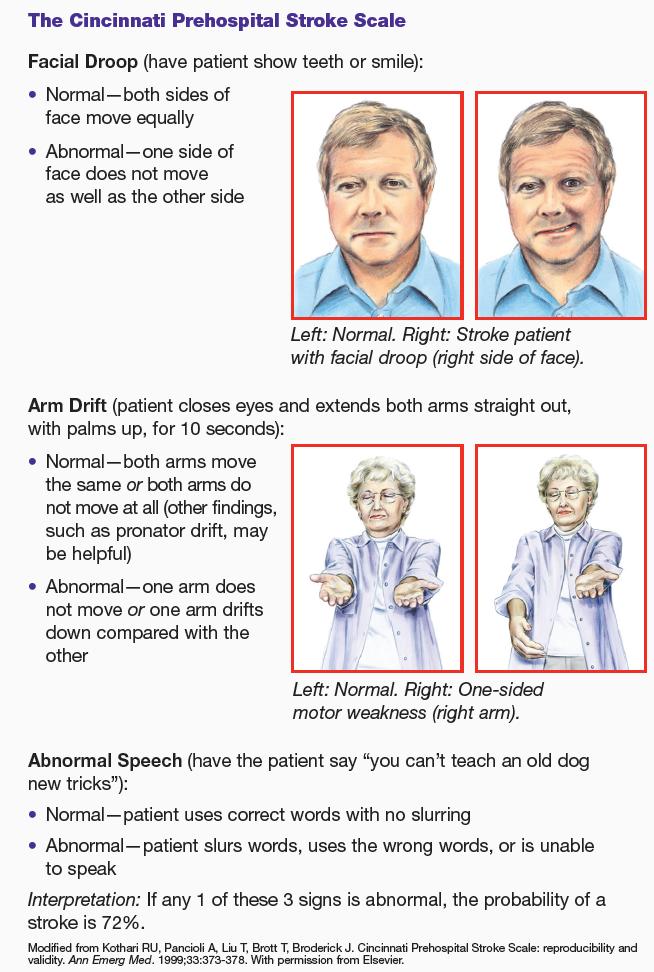
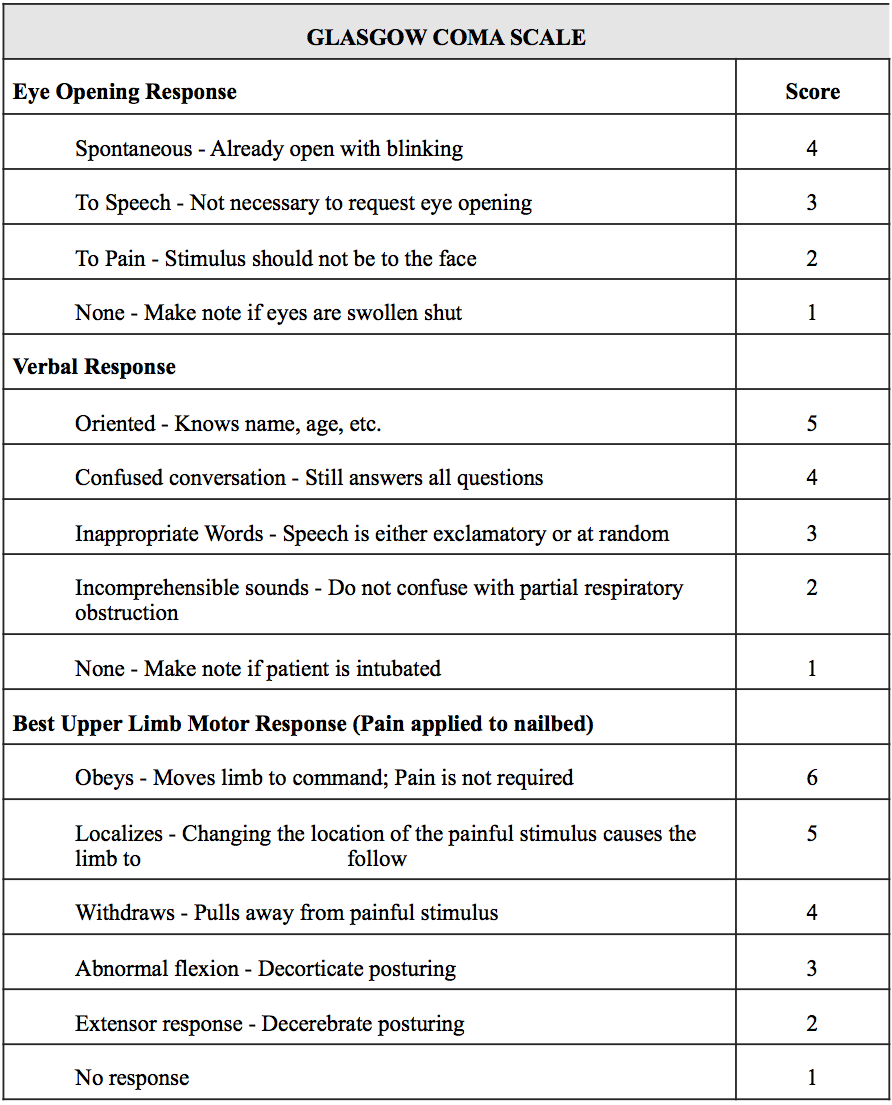
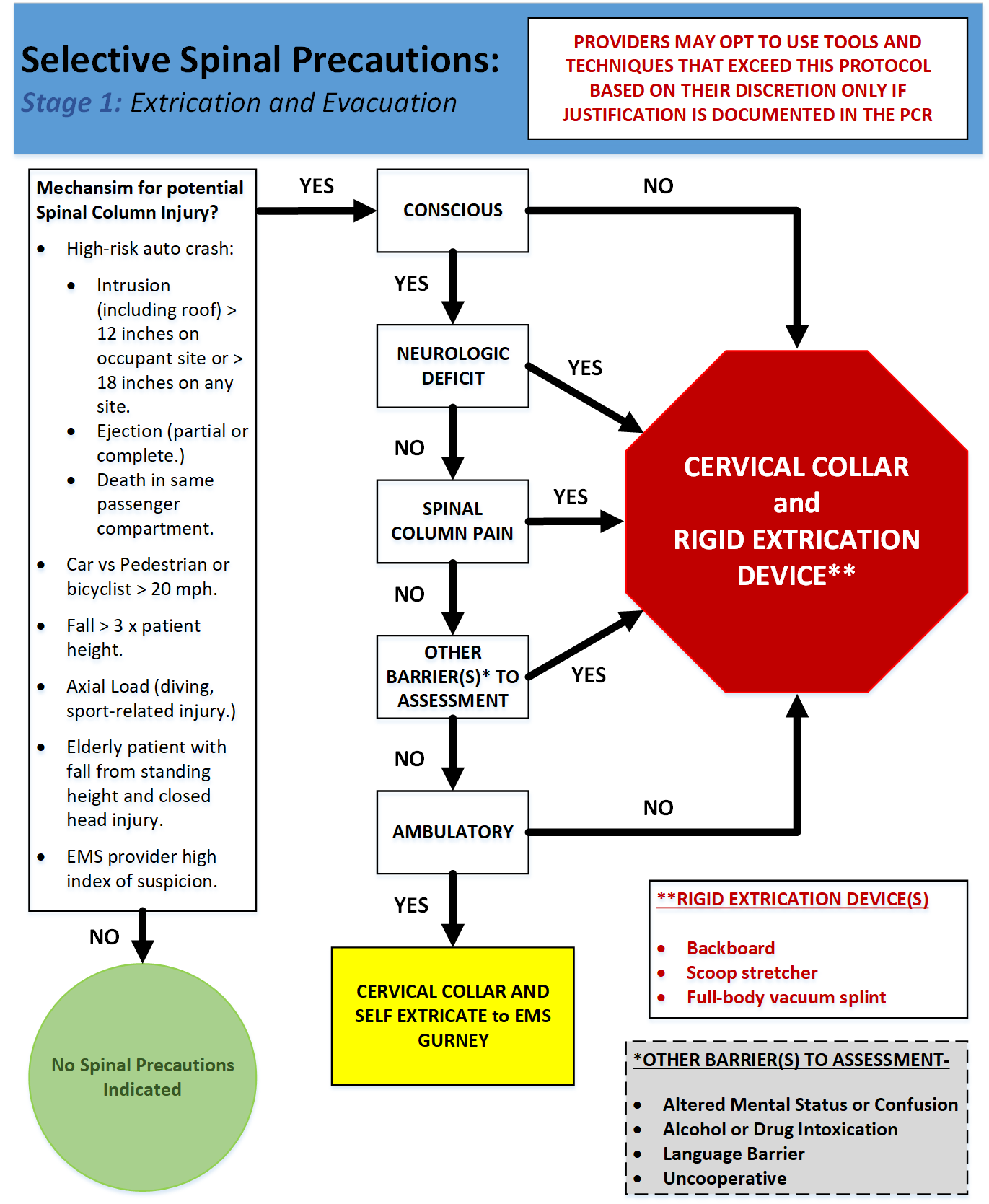
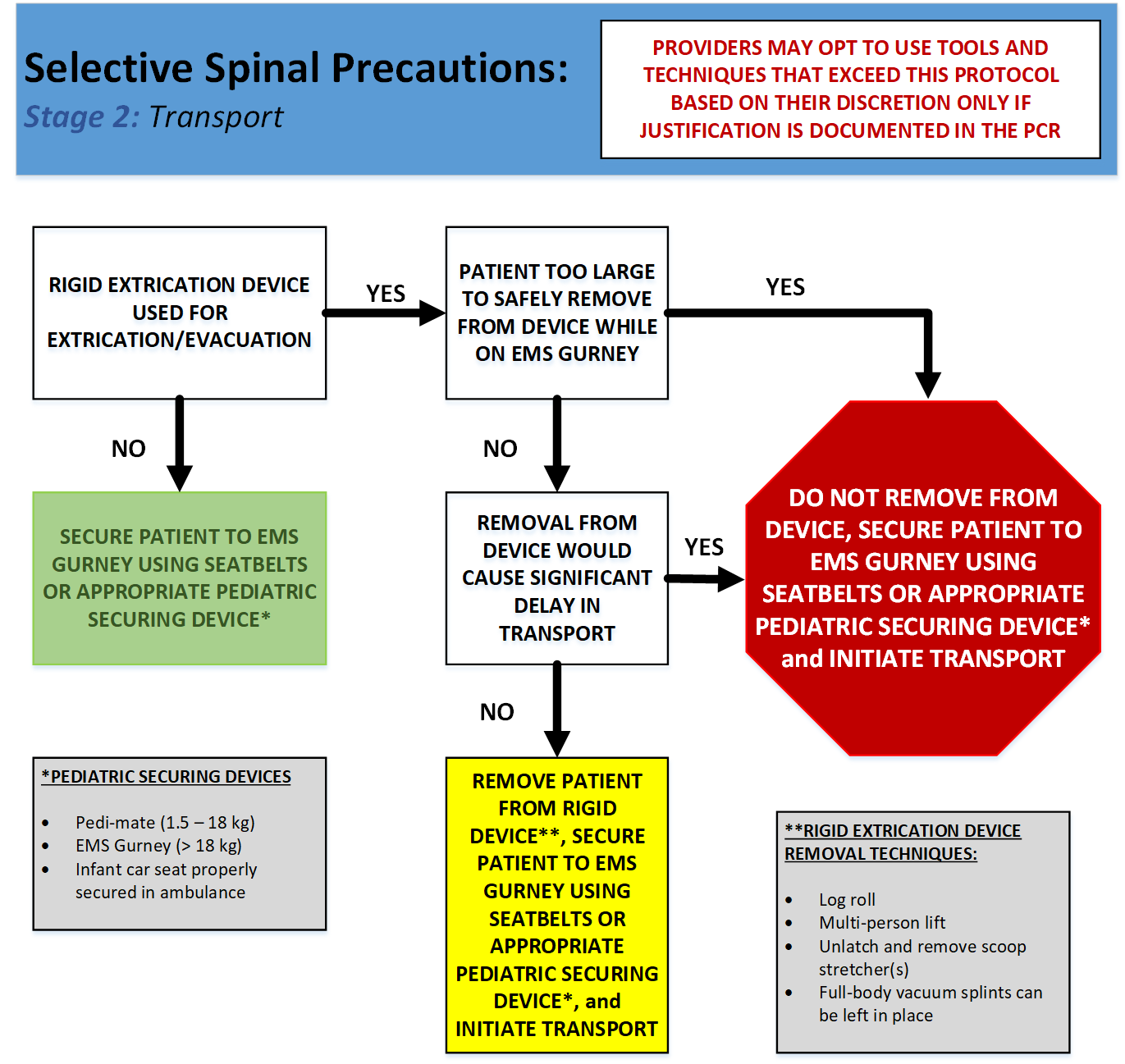
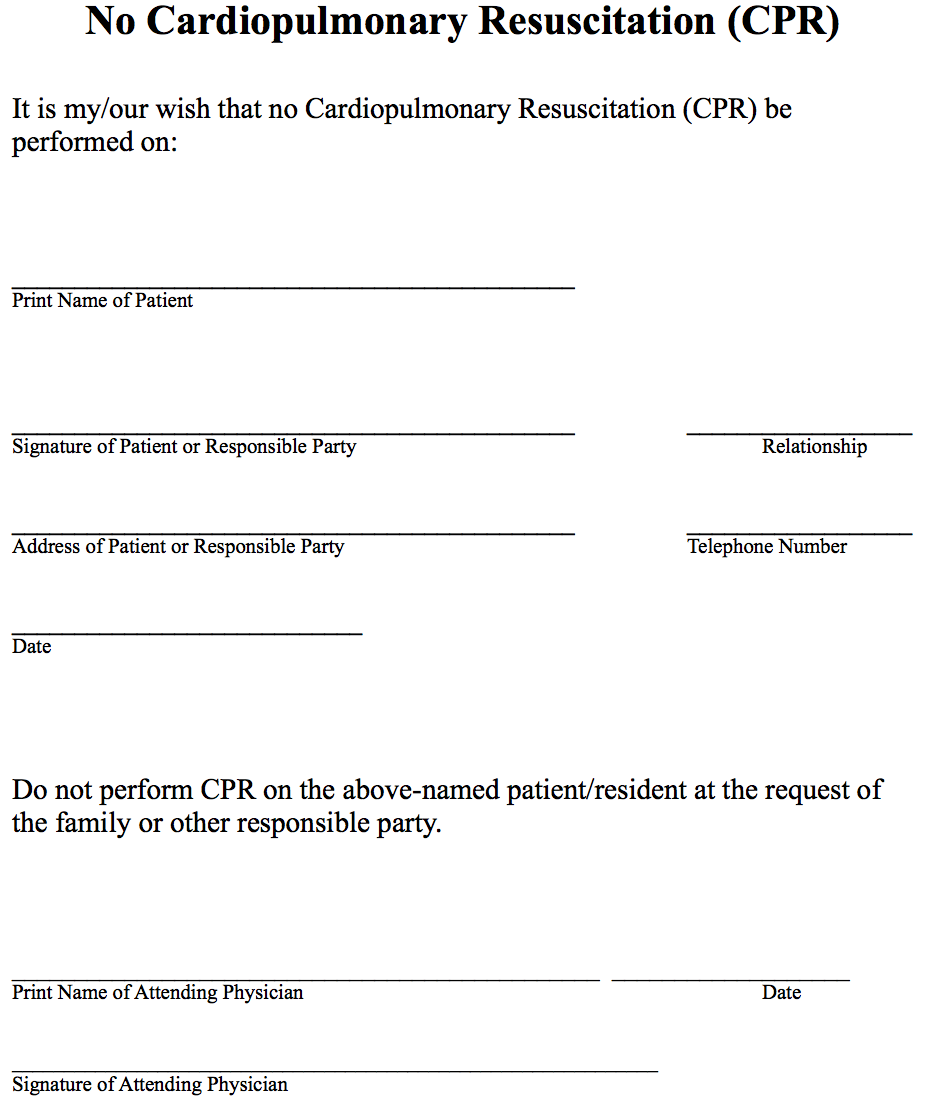
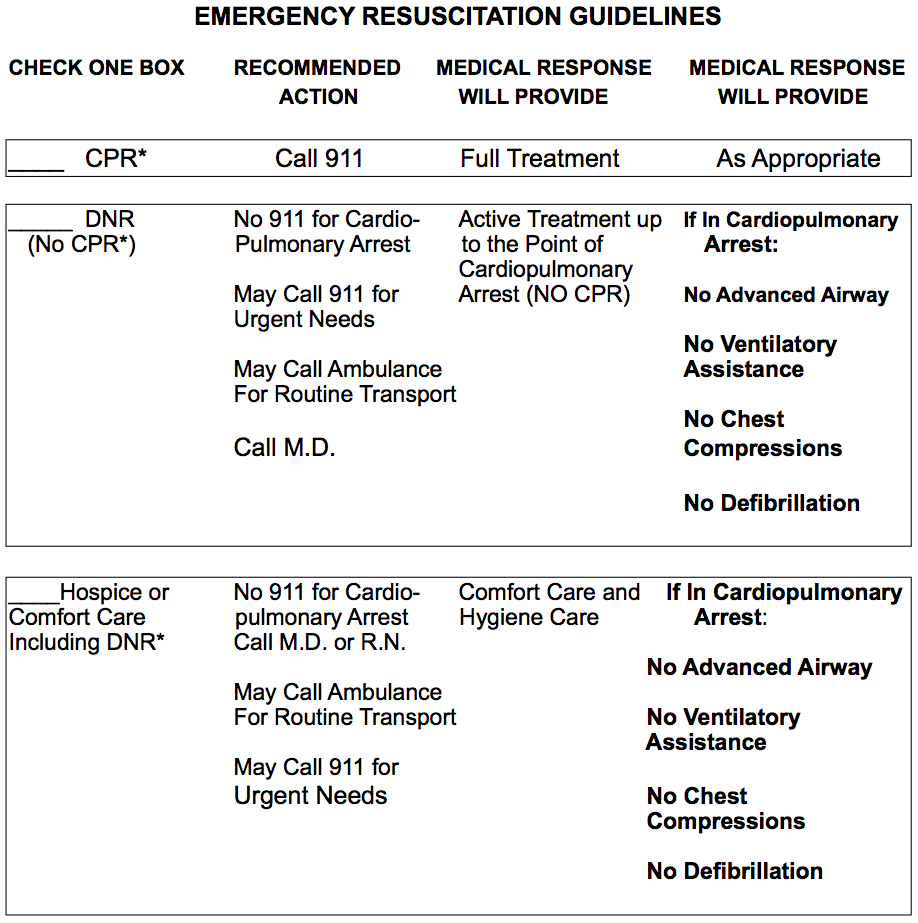
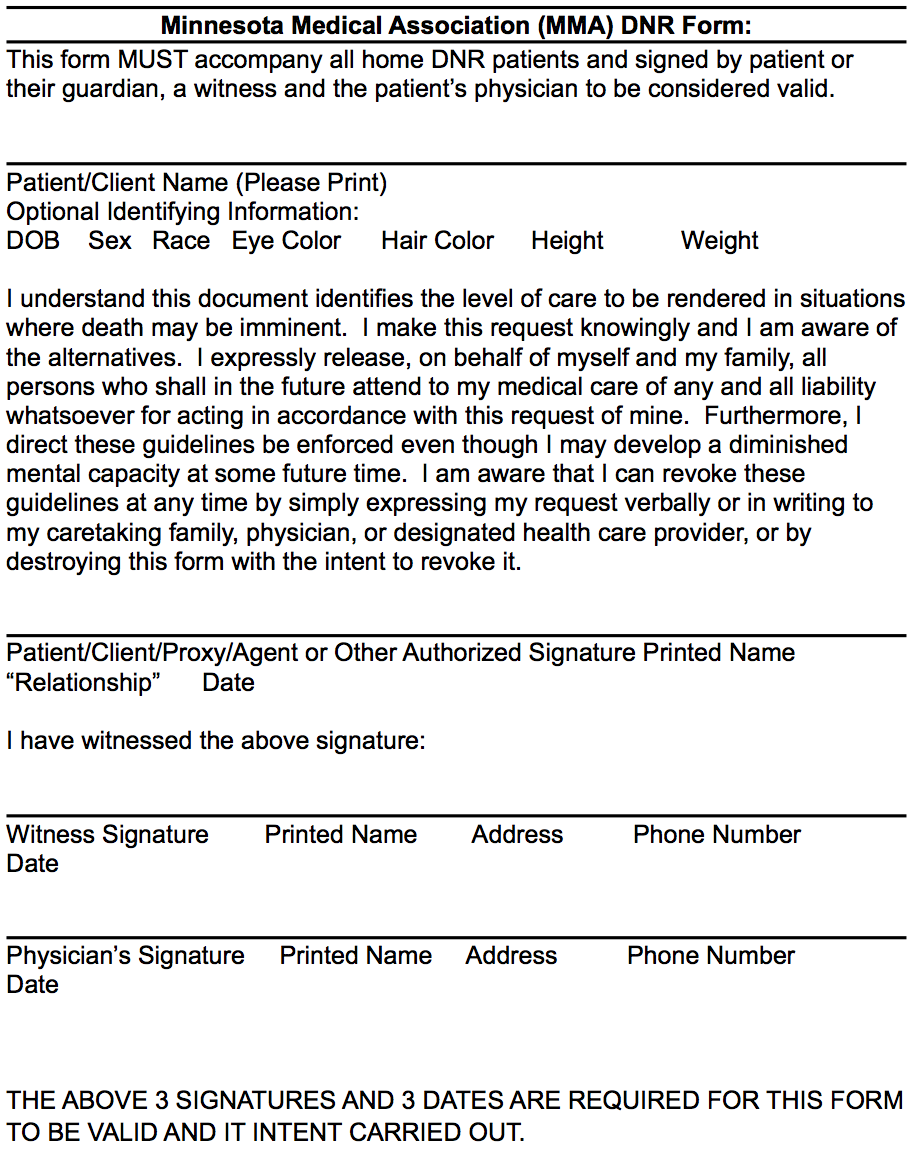
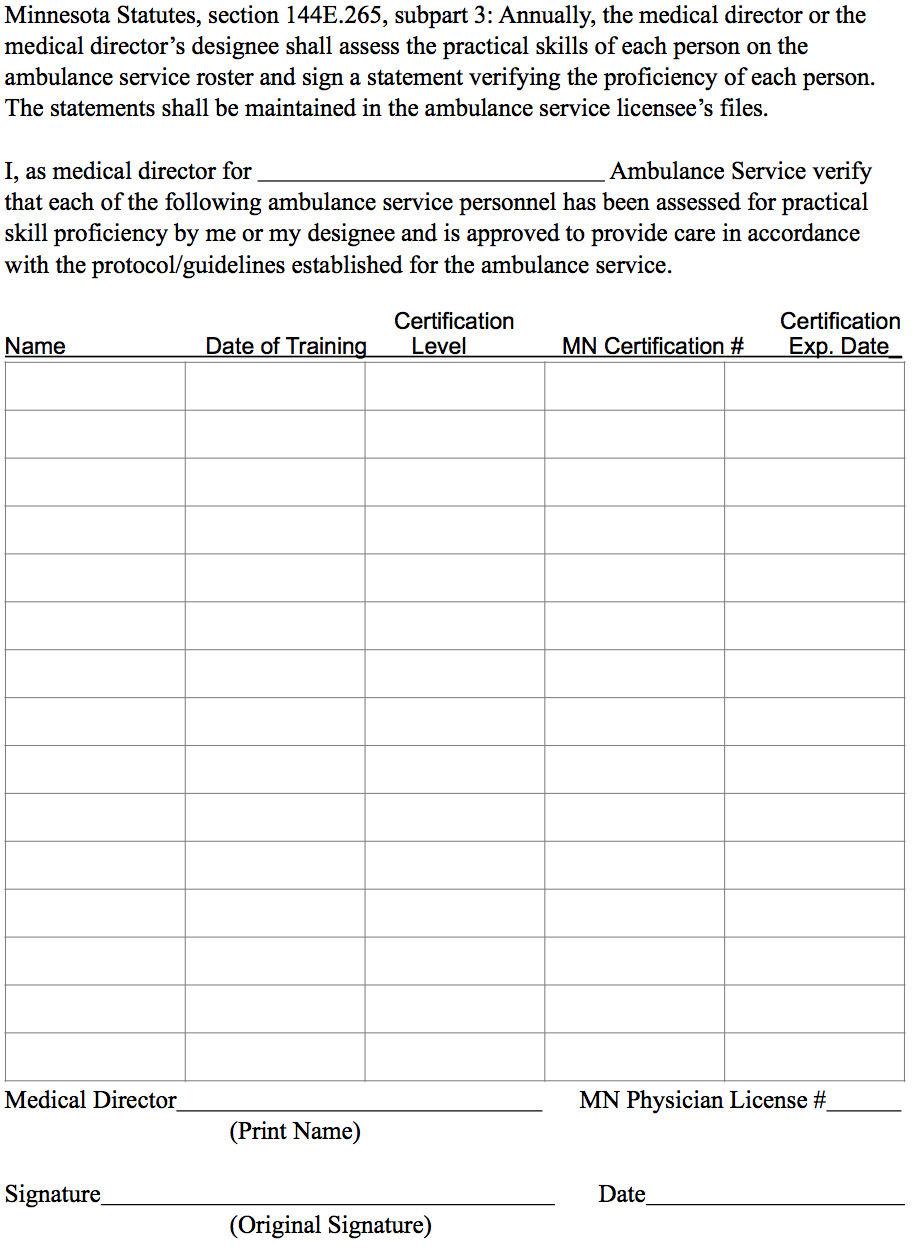
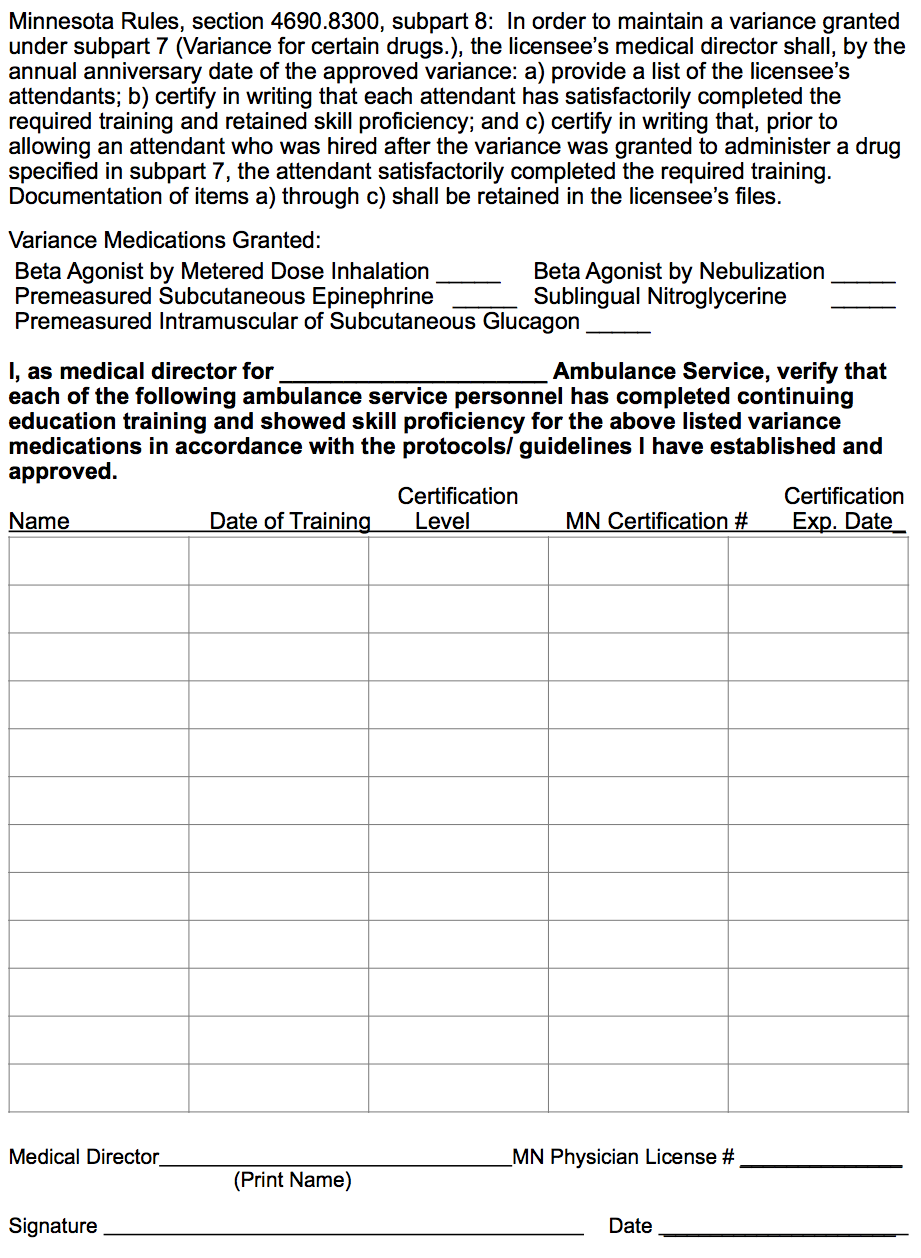
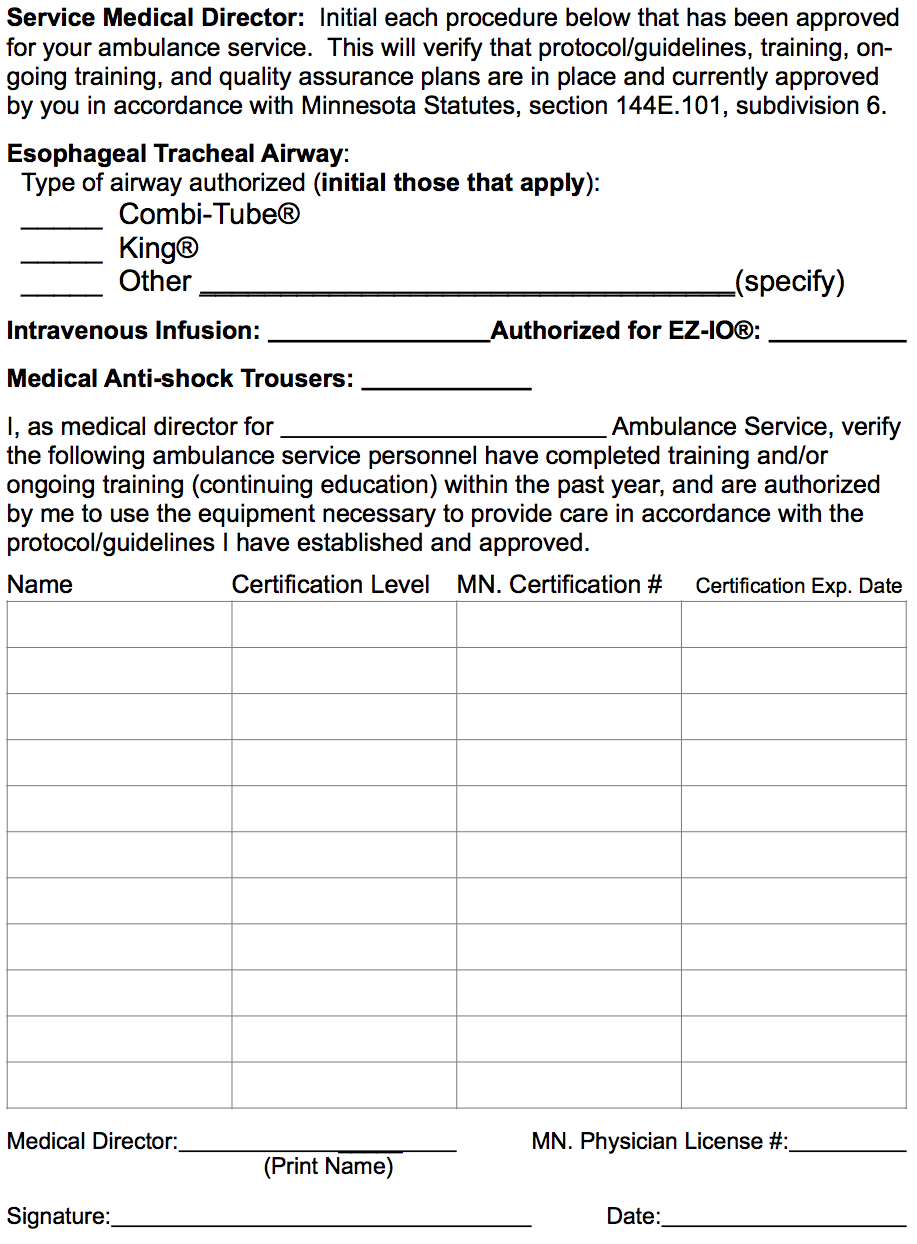
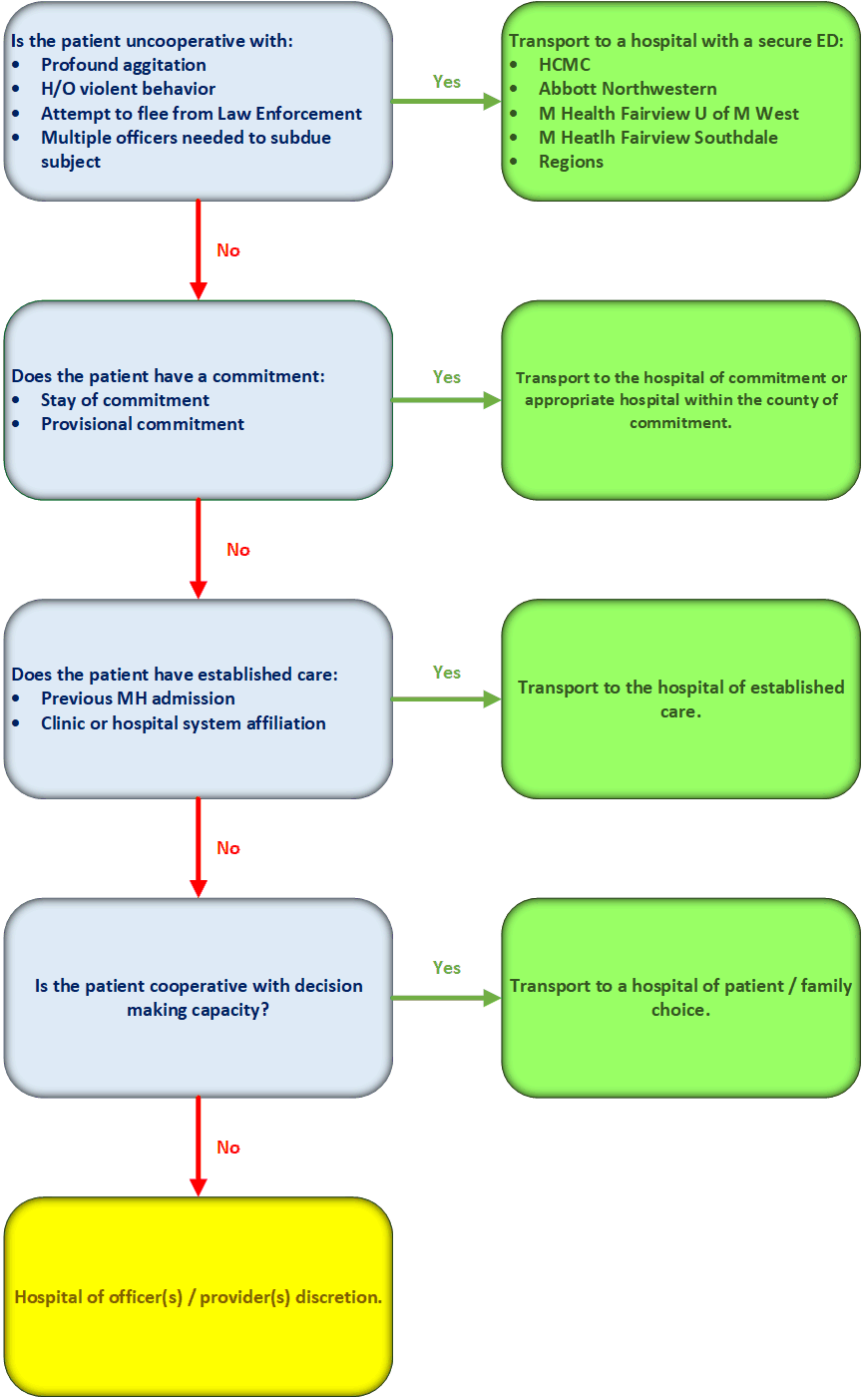
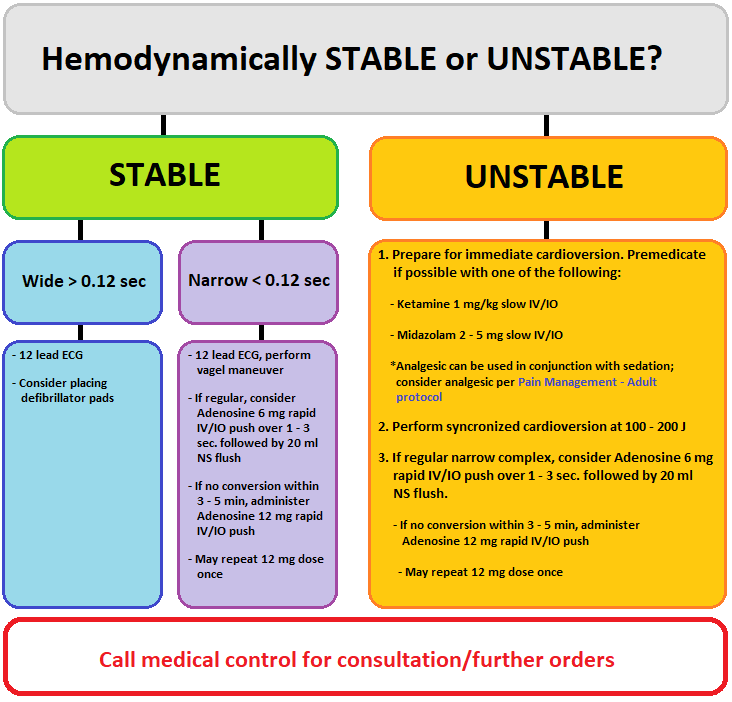
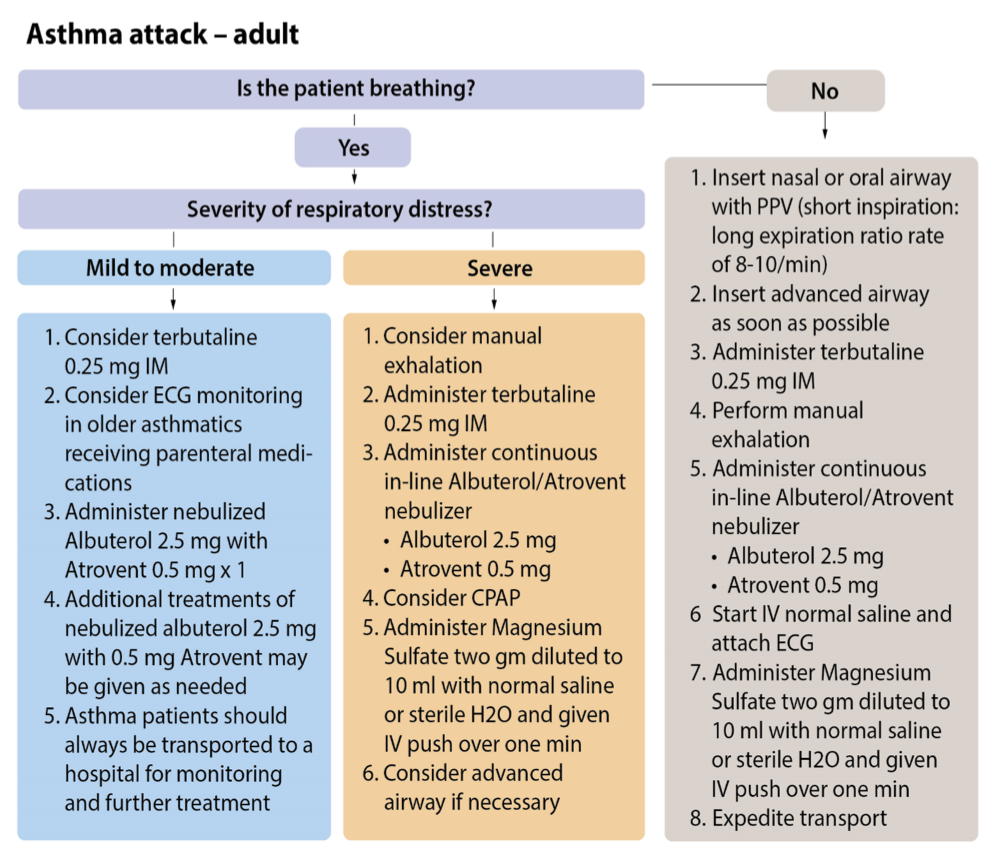
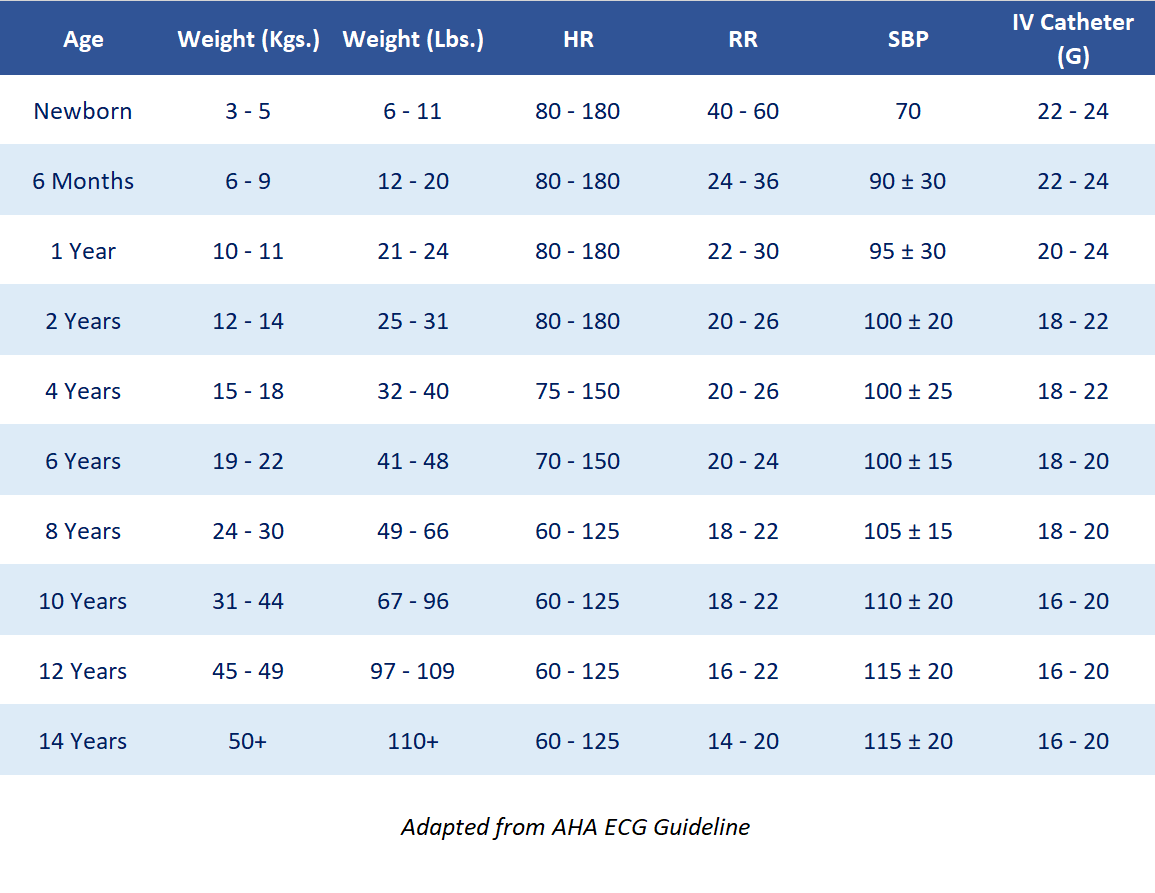
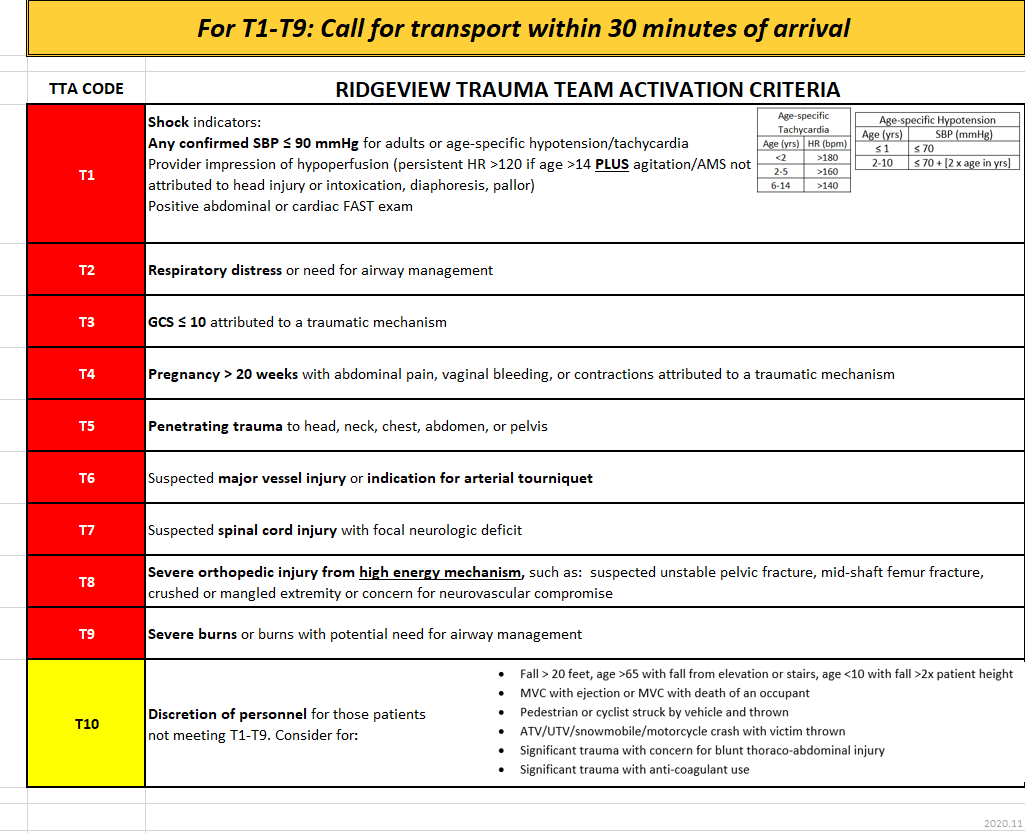
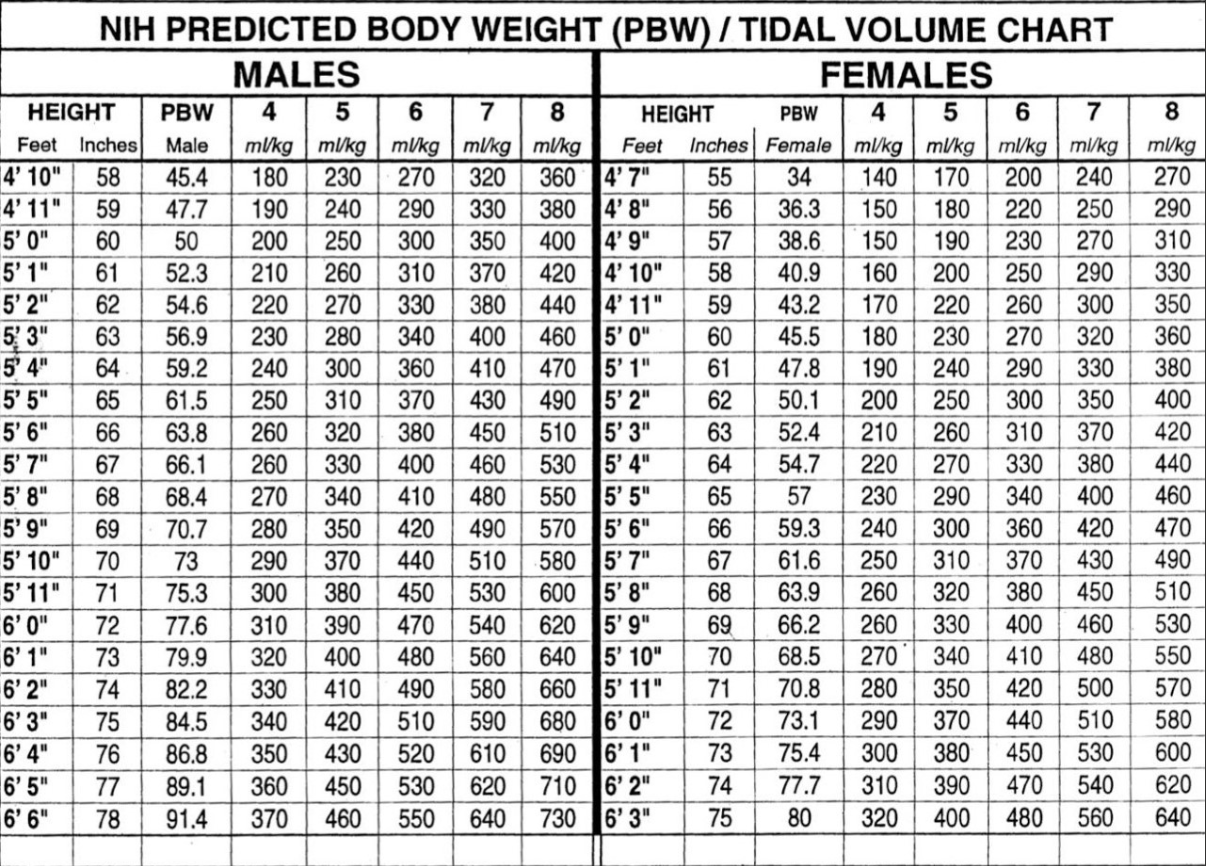
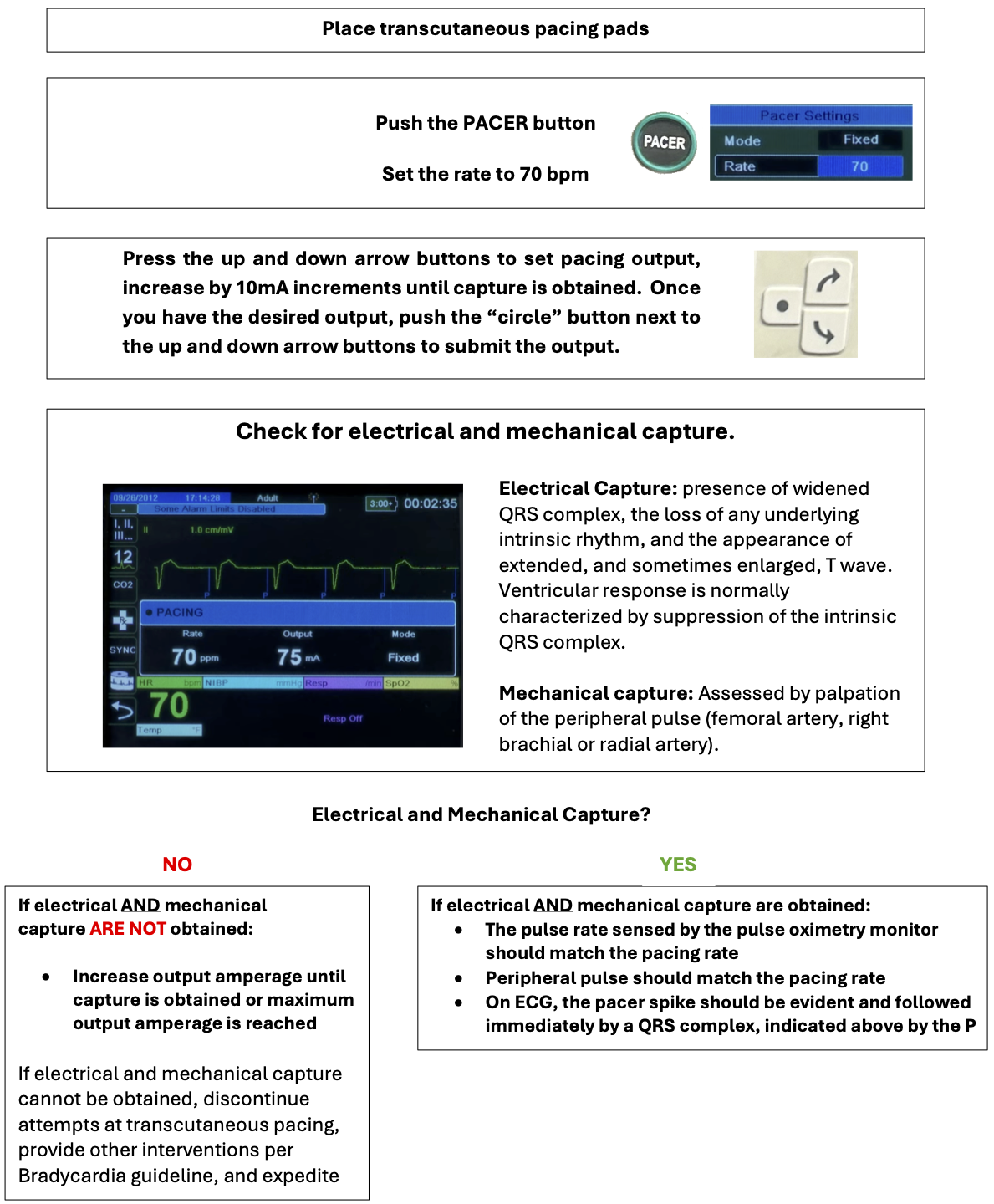
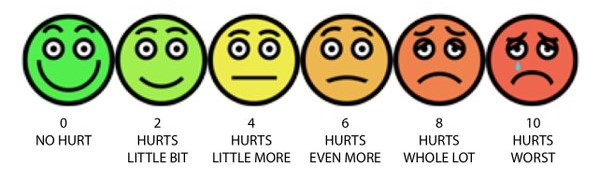
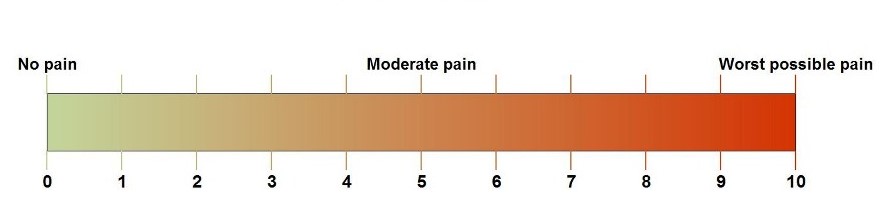
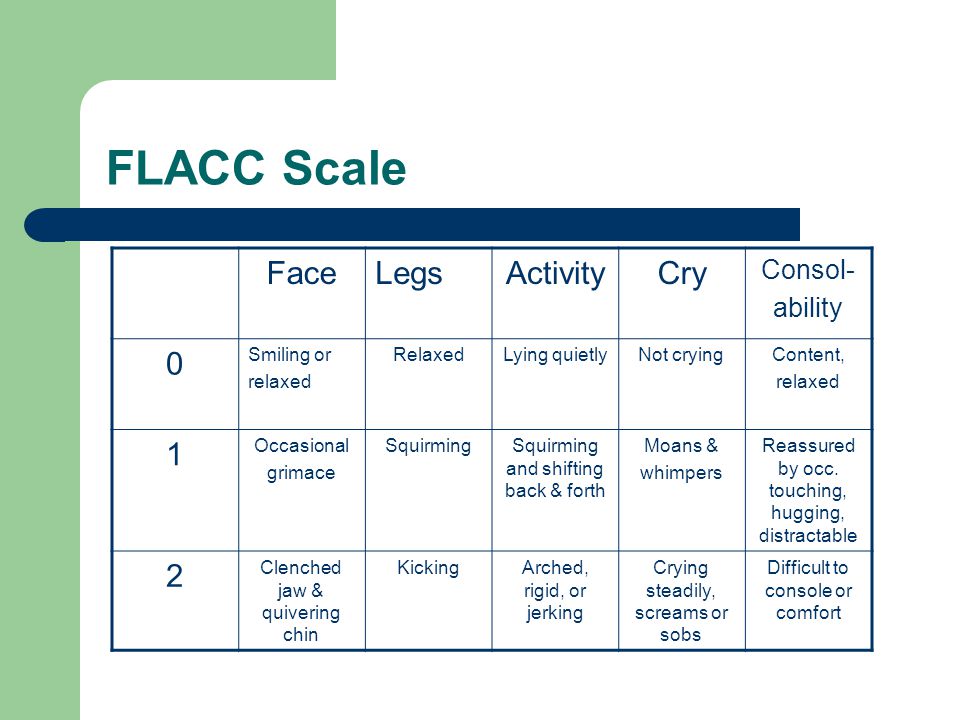
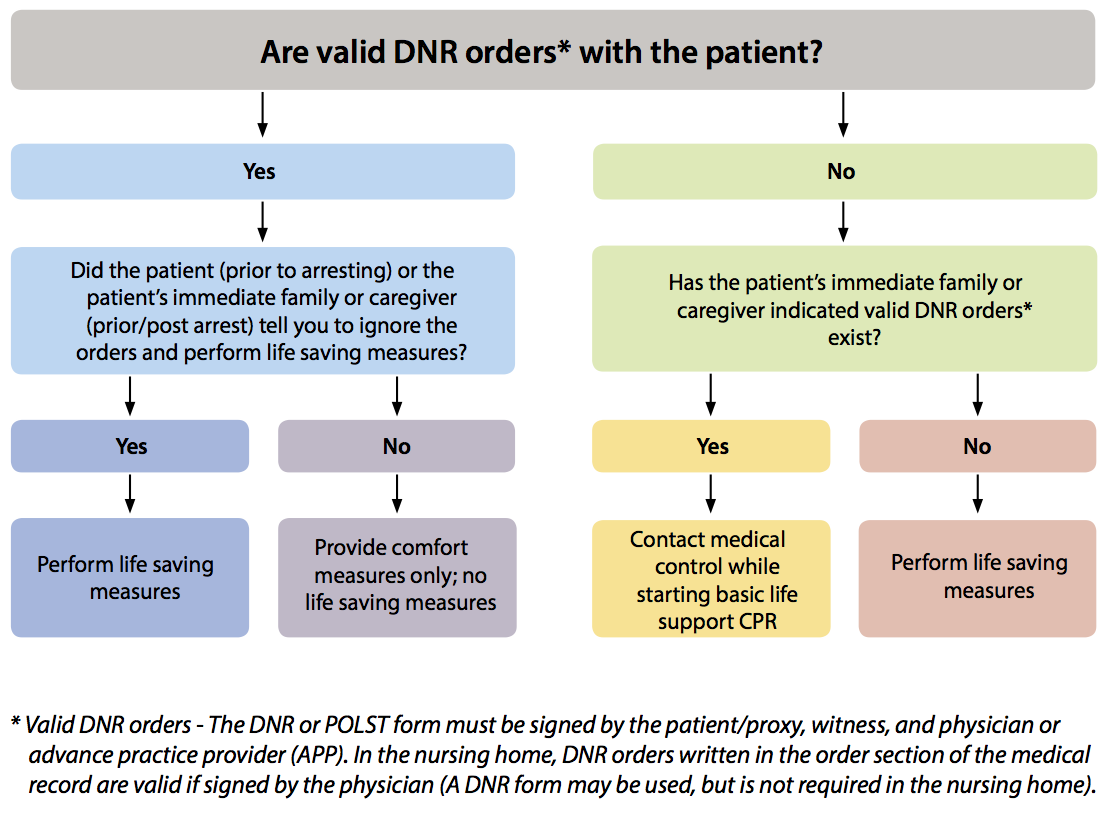
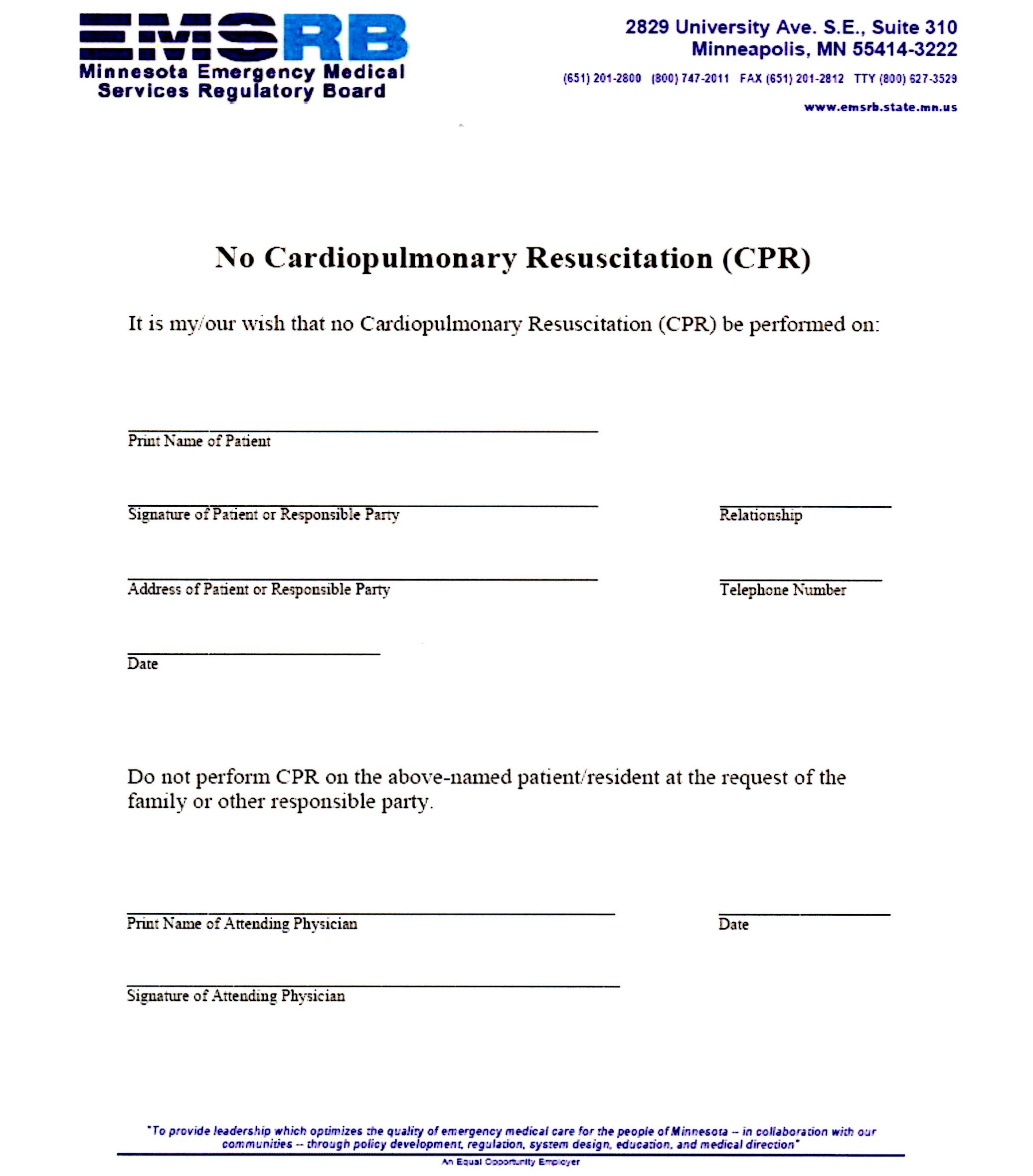
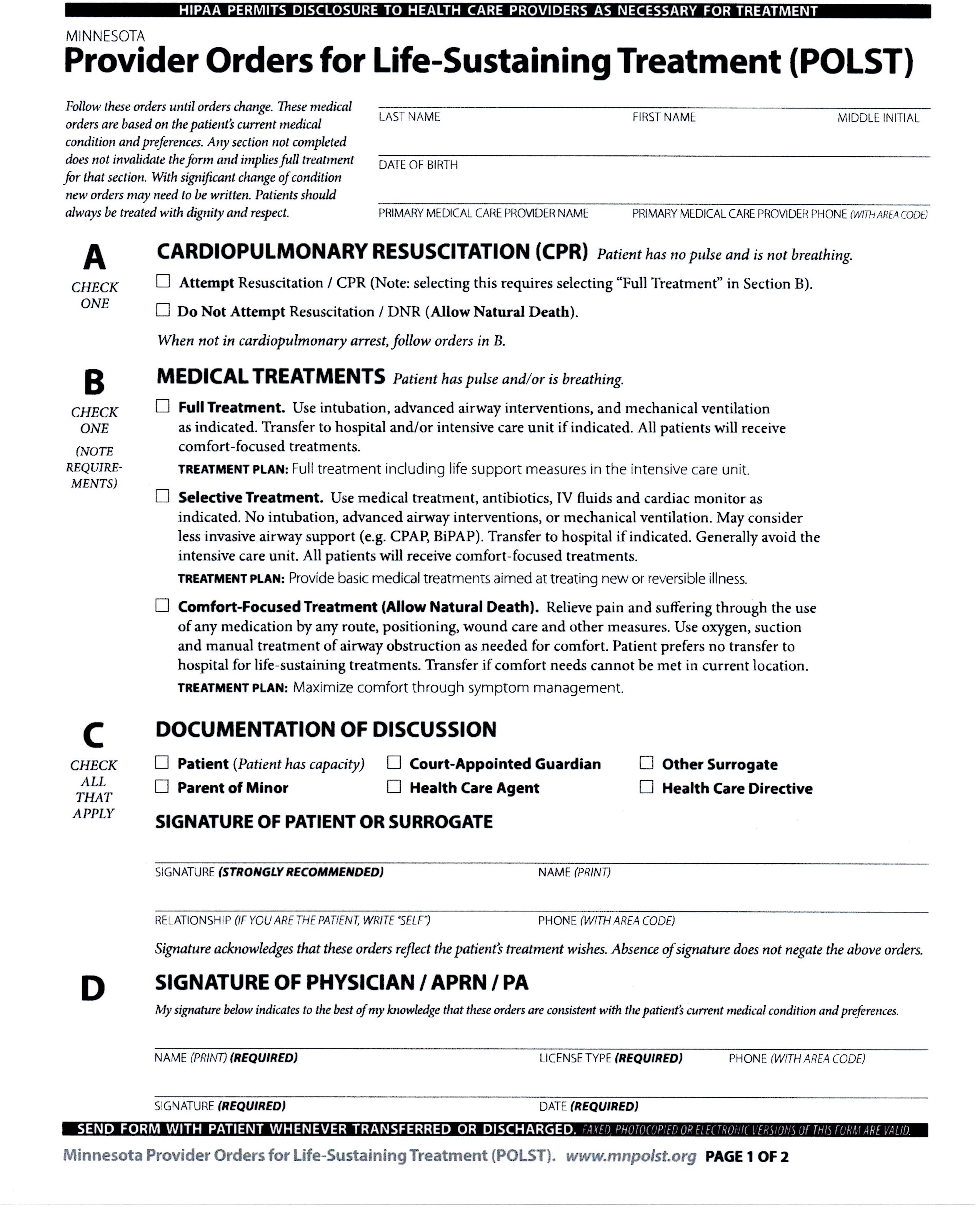



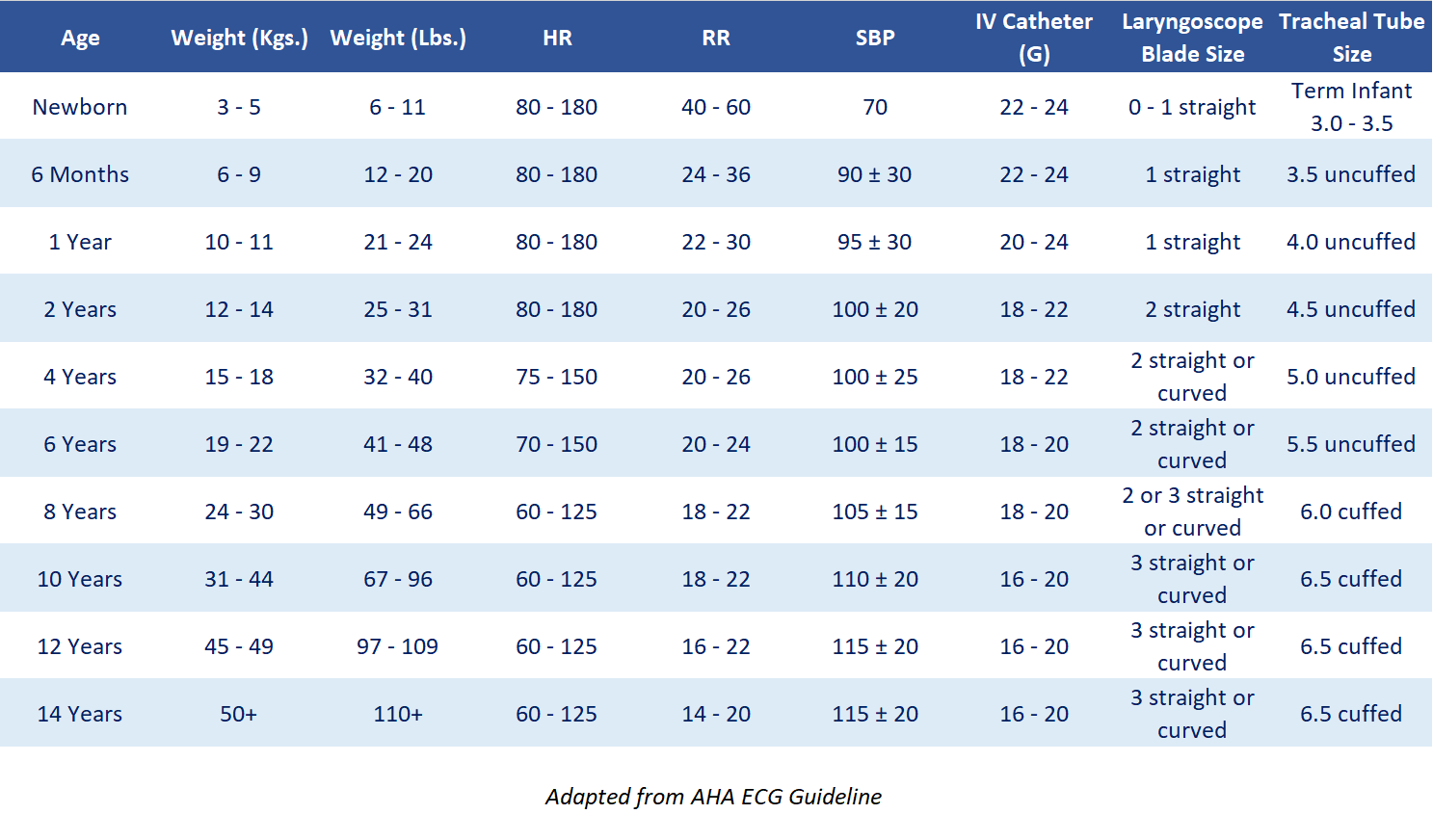

 to highlight ‘Zero Probe’ on the bottom of the screen
to highlight ‘Zero Probe’ on the bottom of the screen ,
this opens up the P1 menu
,
this opens up the P1 menu